
記住我


A total of 147 patients (88 male, 59 female) were enrolled across all three hospital sites (Table 1). Participant ages ranged from 2 to 78 years, with 56 participants (38.1%) under 12 years of age, 13 (8.8%) between 12 and 18 years, 71 (48.3%) between 18 and 65 years, and 7 (4.8%) above 65 years of age. Five different ethnicities were represented in the study, with the majority of participants at each location and in the overall study (122, 83.0%) identifying as Iban.
Table 1 Demographic and household characteristics of patients with febrile illness enrolled across three hospitals in Sarawak, Malaysia, between February and October 2019 (n = 147)Many participants lived in longhouses (78, 53.1%), with 49 (33.3%) reporting residency in houses, and 20 (13.6%) in wooden huts. Households frequently reported obtaining drinking water from multiple sources; 65 (44.2%) collected water from the river, 72 (49.0%) had water piped into their homes, 17 (11.6%) used rain water, and 10 (6.8%) had gravity feed water systems. River water was the most common drinking water source for participants enrolled at Kapit Hospital (55, 53.9%), while participants from Sarikei and Sibu Hospital more commonly reported using piped water (14 per site, 58.3 and 66.7%, respectively).
Among the study population, 34 (23.1%) had not completed any level of formal schooling, while 57 (38.8%) had completed primary and 49 (33.3%) completed secondary schooling. Only 7 (4.7%) participants had gone on to complete college or further professional studies. Among the 78 participants greater than 18 years of age, 46 (59.0%) were involved in occupations associated with high risk of leptospirosis infections, including agriculture (n = 29), fishing (n = 17), hunting (n = 11), and logging (n = 9). Many participants participated in multiple such activities. Within the study population, 52.6% of individuals greater than 18 years of age reported wearing closed-toe shoes for work (n = 41), while 30.8% wore open-toed shoes or sandals. Other reported personal protective equipment (PPE) usage included gloves (14.1%), eye protection (5.1%), and face masks (9.0%).
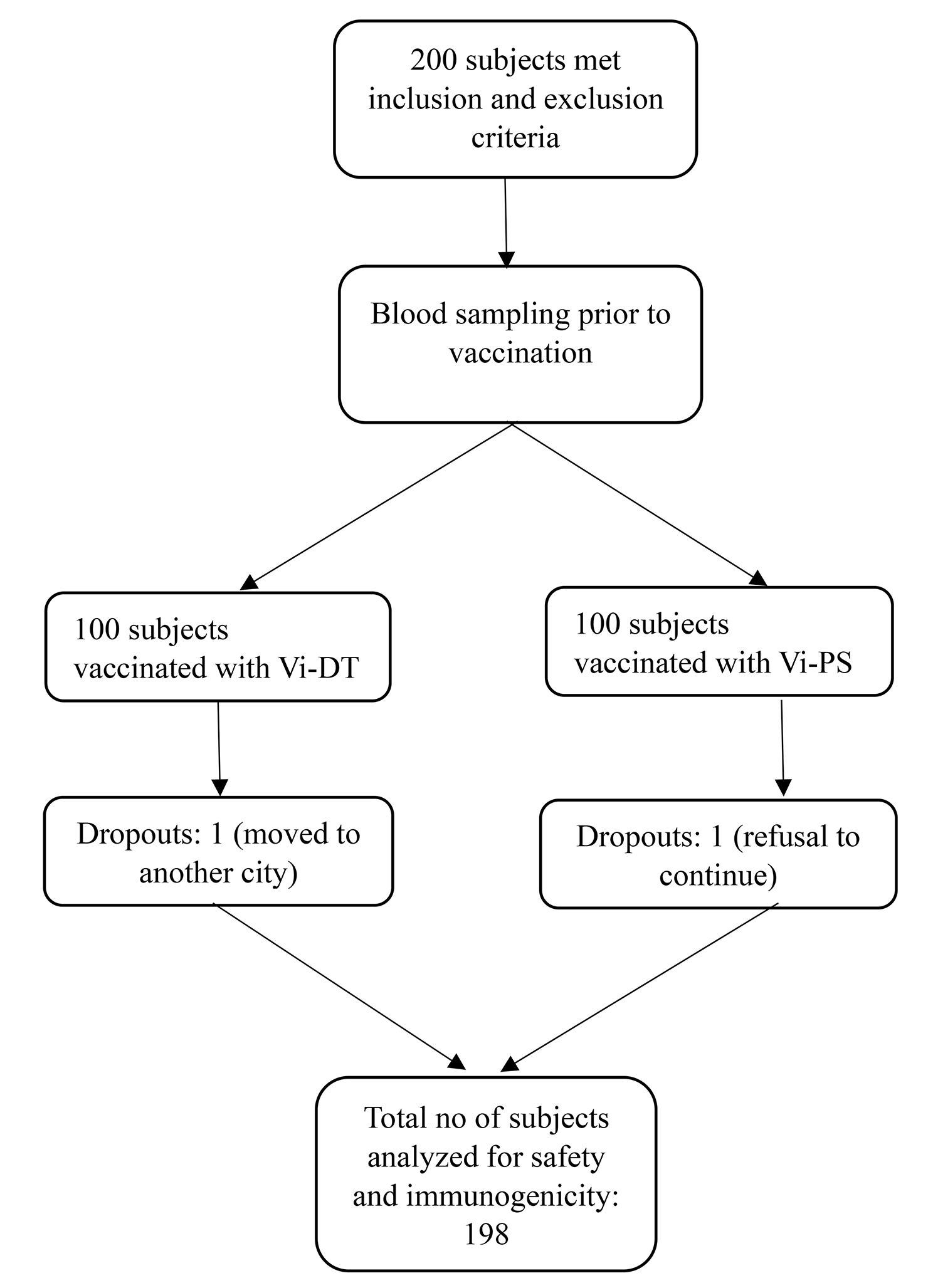
Leptospirosis prevalenceSerological RDT and ELISA results were available for all 147 patients, with calculated prevalences of 42.2% and 15.0% respectively. Out of 62 positive RDT sera specimens, 53 were sent for confirmatory MAT results, along with 5 inconclusive RDT samples and 1 negative. Regardless of RDT outcome, 15/59 (25.4%) sera samples returned positive MAT results. Per our positivity criteria (at least two out of three serological tests positive), a total of 23 participants (15.6%) were considered serology-positive for leptospirosis, of which thirteen participants also presented molecular evidence of leptospires in either sera or urine (Fig. 1).
Fig. 1
Comparison of positive serological leptospirosis results for patients presenting with febrile illness to study hospitals in Sarawak, Malaysia according to various diagnostic methods used. Participants were defined as having leptospirosis if at least two out of three serological tests were found to be positive and/or molecular evidence of Leptospira was identified through qPCR in either participant sera or urine. * RDT: Rapid diagnostic test, Leptorapide latex agglutination test (Linnodee, Ltd., Antrim, Northern Ireland). † MAT: Microagglutination testing, as carried out by the Institute of Medical Research reference lab in Kuala Lumpur, Malaysia, only partial results available. ‡ ELISA: Leptospira IgM ELISA assay (PanBio, Queensland, Australia)
Two sera samples did not have sufficient volume to complete qPCR testing. Among 145 remaining sera and 141 matched urine specimens, a total of 45 leptospirosis infections were identified through qPCR (positive for either sera and/or urine). Evidence of Leptospira was found in 20 (13.8%) sera and 33 (23.4%) urine specimens.
Taken together, serological and molecular testing identified 55 patients with leptospirosis, resulting in an estimated prevalence of 37.4% (55 out of 147) within our study population (Table 2). At Kapit Hospital, 34 of 102 patients (33.3%) were considered positive for leptospirosis, as compared to 9 of 24 (37.5%) at Sarikei Hospital, and 12 of 21 (57.1%) at Sibu Hospital.
Table 2 Leptospirosis prevalence estimates among study population (n = 147) at three enrolling hospitals, Sarawak, Malaysia, according to various diagnostic tests employed. Participants were defined as having leptospirosis if at least two out of three serological tests were found to be positive and/or molecular evidence of Leptospira was identified in either participant sera or urineDiagnostic accuracyLeptorapide RDT analysis on patient sera samples identified 62 (42.2%) as positive, 67 (45.6%) as negative, and 18 (12.2%) inconclusive. RDT analysis on urine identified 43 specimens (30.5%) as positive and 98 (69.5%) as negative. Sensitivity, specificity, PPV, and NPV were assessed for each set of RDT analyses, using combined qPCR results for sera and urine as the gold standard (Table 3). MAT results were primarily available for RDT positive samples, and thus excluded from the diagnostic accuracy calculations to avoid bias; of note, 45.8% of MAT results were inconclusive, as compared to 25.4% positive and 28.8% negative findings (Supplemental Fig. 1). Results of the Leptorapide RDT were further compared to specimen-specific qPCR results.
Table 3 Diagnostic accuracy of Leptorapide latex agglutination test (Linnodee, Ltd., Antrim, Northern Ireland) using acute sera and urine specimen, in comparison to real-time PCR (qPCR)The IgM ELISA assay identified 22 positive (15.0%), 113 negative (76.9%), and 12 equivocal specimens (8.2%). Sensitivity, specificity, PPV, and NPV of the IgM ELISA assay were calculated in comparison to combined qPCR results for sera and urine, as well as for sera-specific qPCR results (Table 4). As before, MAT results were excluded from this analysis.
Table 4 Diagnostic accuracy of Leptospira IgM ELISA assay (PanBio, Queensland, Australia) using acute sera specimen, in comparison to real-time PCR (qPCR)Molecular characterizationSecY sequencing was performed on samples showing PCR amplification and a clean band of the expected size (549 bp) on gel electrophoresis. Samples successfully sequenced (n = 4) originated from urine specimen collected within five days of fever onset. After cleaning and trimming, we compared the 410-bp fragments to secY sequences available from the MLST database (https://pubmlst.org/organisms/leptospira-spp) and identified Leptospira interrogans as the infecting species (GenBank accession numbers are provided in Supplemental Table 1). When compared to a worldwide database including 134 secY sequences of Leptospira interrogans [20], our four sequences were identical or closely related to leptospires identified in Malaysia, Indonesia, India, the Philippines and China.
Disease presentationAmong the 55 defined leptospirosis patients, 9.1% (n = 5) presented with severe disease, characterized by death (n = 1), septic shock (n = 4) and respiratory distress requiring invasive ventilation support (n = 3). Another seven (12.7%) presented with moderate disease requiring non-invasive ventilation support (n = 4), upper gastrointestinal bleeding (n = 1), atrial fibrillation (n = 1) and thrombocytopenia (n = 2). The remaining 43 patients (78.2%) presented with mild disease. Acute kidney injury and transaminitis were observed at all disease severity levels (34.5% and 32.7% respectively).
The most commonly self-reported symptoms among the leptospirosis-positive patients were fever (52, 94.5%), nausea or vomiting (39, 70.9%), headache (37, 67.3%), and chills (36, 65.5%) (Supplemental Table 2). Several patients reported experiencing myalgia (29, 52.7%), joint pain (26, 47.3%), or conjunctivitis (17, 30.9%), while lethargy and diarrhea were uncommon (3, 5.5% and 9, 16.4%, respectively). Notably, jaundice was not observed in any of the leptospirosis positive patients.
Of note, two additional study participants died during the course of their hospitalization, but we found no detectable evidence of Leptospira infection in either of their samples.
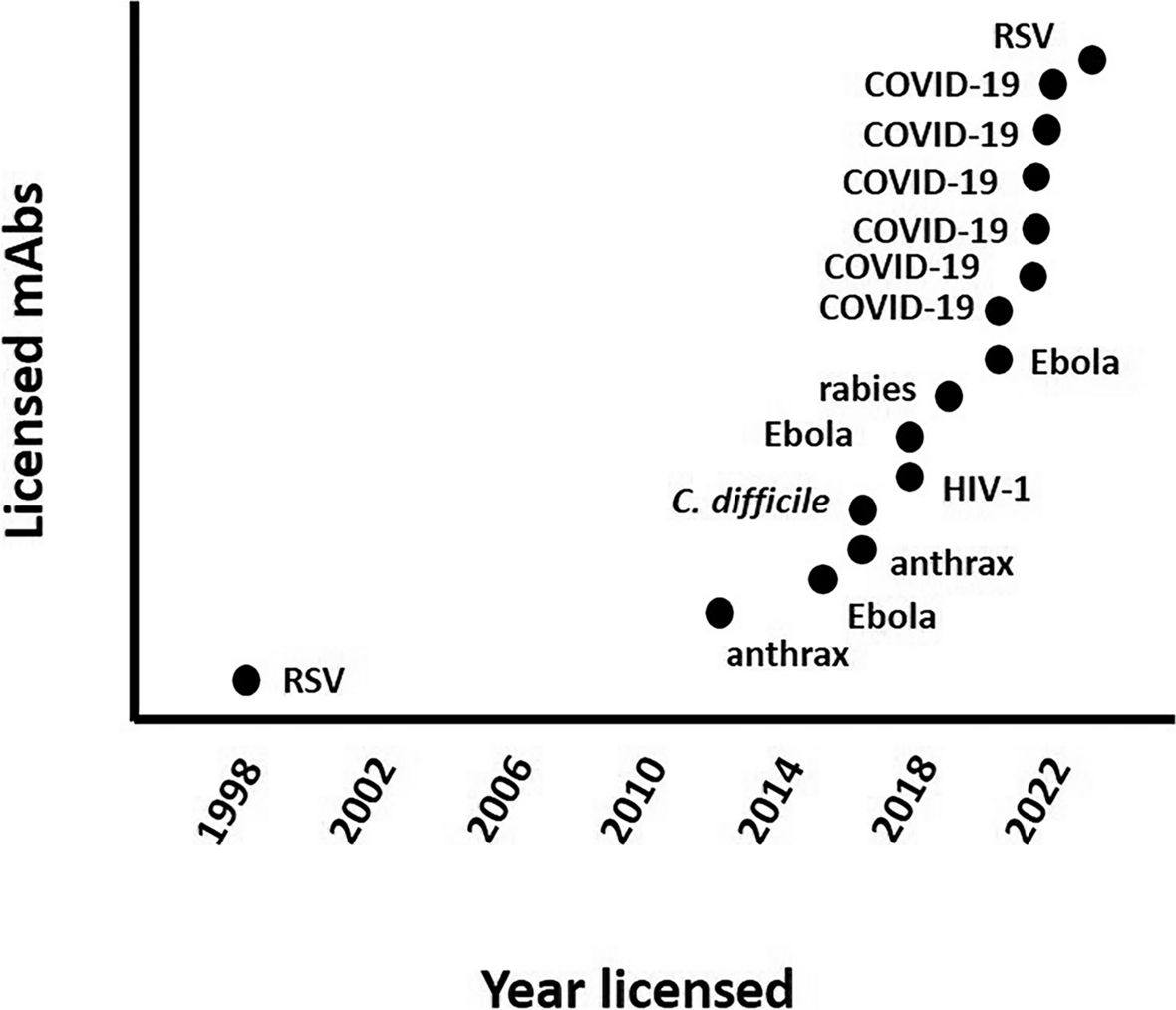
Symptom onsetLeptospirosis-positive patients generally presented in the early phase of the disease, indicating that they were likely in the acute stage of infection at the time of sample collection (Fig. 2). Overall, 47 of 55 defined positive patients (85.4%) were enrolled within 6 days post symptom onset (DPSO; self-reported), with five (9.1%) presenting on day 7 and one (1.8%) on day 8. Two patients did report having experienced joint pain and myalgia, among other symptoms, for 14 days.
Fig. 2
Days post symptom onset (DPSO) at the time of enrollment, as self-reported by leptospirosis patients (diagnosis determined by molecular and/or serological evidence). The acute phase typically takes place in the first week of illness, followed by antibody development 5–7 days post symptom onset
Comparatively, patients considered negative for leptospirosis reported having experienced non-specific febrile symptoms from one to 28 days prior to sample collection.
Correlation calculations identified sera and urine specimen qPCR analysis as complementary (Supplemental Table 3). Of the 45 participants with molecular evidence for leptospirosis, 12 (26.7%) were qPCR positive only through sera analysis, 25 (55.6%) only through urine, and 8 (17.8%) had Leptospira positivity in both sample types (Table 5). Sera-based qPCR results primarily picked up evidence of Leptospira presence between 2 and 6 DPSO, with one patient testing positive with no documented fever (Fig. 3). Urine-based qPCR results were positive between 1 and 8 DPSO, with three patients testing positive with no documented fever (Fig. 4).
Table 5 Likely phase of disease progression for leptospirosis qPCR-positive patients as defined by sample positivity in sera and/or urine specimens. Participants with Leptospira evidence only in sera were classified to be in the onset phase, those with evidence in both sera and urine were classified in the dissemination phase, and those with evidence only in urine were classified in the excretion phaseFig. 3
Evidence of leptospirosis in sera specimens from different diagnosis methods and according to patient-reported time of fever duration at time of sampling. Diagnosis determined by real-time PCR analysis, Leptorapide latex agglutination test (Linnodee, Ltd., Antrim, Northern Ireland), or Leptospira IgM ELISA assay (PanBio, Queensland, Australia)
Fig. 4
Evidence of leptospirosis in urine specimens from different diagnosis methods and according to patient-reported time of fever duration at time of sampling. Diagnosis determined by real-time PCR analysis or Leptorapide latex agglutination test (Linnodee, Ltd., Antrim, Northern Ireland)
Participants with serological evidence for leptospirosis (n = 23) were identified from 1 to 8 DPSO, with one identified at 14 DPSO and one reporting no fever. Among these, the ten patients with no molecular evidence of Leptospira were primarily identified between 2 and 7 DPSO, with one patient presenting at 14 DPSO.
Independently of other serological assessments, the Leptorapide RDT provided positive results for patients 1 to 20 DPSO using sera samples and 1 to 14 DPSO using urine samples. The majority of the urine-based RDT positive results were within 1 to 7 DPSO, with 1 specimen positive at 10 DPSO and another at 14.
The IgM ELISA assay detected antibody evidence in patients 2 to 8 DPSO, and in one participant presenting without fever. MAT positives were identified primarily in participants 2 to 7 DPSO, as well as in one participant at day 10, one at day 14, and one presenting without fever.
Risk factor analysisBivariate analyses demonstrated the participant’s completed level of education, type of housing, and frequency of washing clothes in the local river as being associated with leptospirosis diagnosis. Participant ethnicity, occupation, use of PPE, primary water source, and exposure to cats, dogs, pigs, poultry, or rodents were not found to be significantly associated with leptospirosis diagnosis, nor was the enrollment site, recent flooding, engaging in other river-based activities, household income, or primary mode of transportation (Supplemental Table 4).
Multivariate analysis identified completing primary school and weekly washing of clothes in the local river as most predictive of a positive leptospirosis result in sera and/or urine. In this joint model, participants who had completed primary school were more than twice as likely to test positive for leptospirosis infection when compared to those with no education (OR 2.5, 95% CI 1.0–6.4). Those who completed secondary school were nominally less likely to show evidence of infection than those with no education (OR 0.9, 95% CI 0.4–2.5) (Table 6).
Table 6 Predictive factors for positive leptospirosis diagnosis (having either molecular or serological evidence of leptospirosis) in the study population (n = 147), as calculated through bivariate and multivariate analysesWashing clothes in the local rivers on a daily basis resulted in similar odds of having a leptospirosis diagnosis when compared to those who reported never washing clothes in the river (OR 0.9, 95% CI 0.3–2.3). In contrast, individuals who washed clothes weekly in the rivers had a tenfold increase in the likelihood of leptospirosis diagnosis, albeit with very low specificity (OR 10.6, 95% CI 1.4–214.8).
Multicollinearity across the model was not identified as a concern, with a mean variance inflation factor of 1.06 for all included variables.
留言 (0)