
記住我


Natalizumab, a recombinant humanized monoclonal antibody directed against the α4 subunit of the integrins α4ß1 (VLA4) and α4ß7, has been approved for the treatment of active relapsing-remitting multiple sclerosis (MS) based on the AFFIRM and SENTINEL phase 3 clinical trials (1, 2). It hinders the transmigration of immune cells into the CNS by blocking the interaction between VLA4, expressed by all leucocytes except neutrophils, and endothelial cells (3).
Analysis of cerebrospinal fluid (CSF) after natalizumab therapy demonstrated its beneficial therapeutic effects: the number of white blood cells (WBC) were found to be decreased (3, 4). Moreover, previous studies have shown increased lymphocyte numbers, predominantly of the B cell lineage, in the peripheral blood after natalizumab therapy (5, 6).
However, there is very limited data on the histopathological changes of the CNS parenchyma after natalizumab therapy. To our knowledge only one histological study has been published, an analysis of a single patient with confounding pathology who developed progressive multifocal leukoencephalopathy (PML) due to natalizumab therapy (7). Therefore, the aim of this study was to provide a detailed histopathological characterization of CNS inflammatory cell infiltration in natalizumab-treated MS patients. For this purpose, tissue samples from 24 natalizumab-treated MS patients were analyzed and the data were compared to disease duration-matched MS controls. To complement the analysis, immune cells in blood and CSF of 30 natalizumab-treated patients were quantified by flow cytometry.
2 MATERIALS AND METHODS 2.1 PatientsThe present study included tissue samples from MS patients who had been treated with natalizumab (labeled as MS + Ntz) and afterward had either undergone brain biopsy (n = 20) or whose tissue samples had been collected at autopsy (n = 4). In the four autopsy cases, the cause of death was a fulminant MS disease course in two patients, cardiac infarction in one and recurrent infections in the other. Brain biopsies were taken for diagnostic reasons, e.g. to rule out progressive multifocal leukoencephalopathy (PML), a known severe side effect of natalizumab treatment, or due to clinical deterioration after stopping natalizumab therapy. Tissue in all patients showed inflammatory demyelinating lesions consistent with MS. Patients with PML and neuromyelitis optica spectrum diseases (NMOSD) were excluded from the study. Testing for JCV, the virus that causes PML, was done by immunohistochemistry (SV40 T Ag (Ab-2); clone: PAb416; Merck Millipore, Massachusetts, USA) and/or in situ hybridization. Of the 24 natalizumab-treated patients, 13 responded to the therapy (labeled as resp.), while 4 patients did not (labeled as non-resp.). Non-response was defined as presenting with relapses and/or new lesion formation on magnetic resonance imaging (MRI) during treatment with natalizumab. In 7 patients, no information on therapy response was available. Controls (labeled as MS) included 21 MS patients with no prior natalizumab therapy, and a disease duration comparable to natalizumab treated patients (n = 11 biopsies and 10 autopsies). Demographic and clinical characteristics of the study participants and MS controls are outlined in Table 1. For blood and CSF analyses, we included 30 natalizumab-treated MS patients and 42 MS controls (Table 1). Lumbar puncture was performed for diagnostic reasons, e.g. to rule out PML.
TABLE 1. Demographic and clinical characteristics of natalizumab-treated MS patients and controls Biopsies Autopsies Blood/CSF Total biopsies Active demyelinating biopsy lesions Inactive demyelinated biopsy lesions Inactive demyelinated autopsy lesions MS + Ntz (n = 20) MS (n = 11) MS + Ntza (n = 17) MS (n = 7) p value MS + Ntza (n = 5) MS (n = 4) p value MS + Ntzb (n = 4) MS (n = 10) p value MS + Ntz (n = 30) MS (n = 42) p value Demographic characteristics Age, years, median (range) 38.5 (23–54) 32 (14–52) 40 (29–52) 32 (14–52) 0.1921 44 (23–54) 33 (28–44) 0.4606 41 (32–62) 47 (28–71) 0.6354 42 (29–61) 37.5 (18–64) 0.2761 Female, no. (%) 14 (70) 9 (81.8) 12 (70.1) 5 (71.4) 3 (60.0) 4 (100.0) 3 (75.0) 4 (40.0) 20 (66.7) 28 (66.7) Clinical characteristics Disease duration, years, median (range) 10 (1.5–23) 7 (5–14) 10 (1.5–23) 7 (5–10) 0.1801 6 (1.5–9) 8 (5–14) 0.3429 10.5 (6–20) 10.5 (2.5–23) 0.7761 11.9 (4–24) 0.9 (0–13) <0.001 RR, no. (%) 15 (75) 6 (54.5) 13 (76.5) 3 (42.9) 4 (80.0) 3 (75.0) 3 (75.0) 0 30 (100) 36 (85.7) SP, no. (%) 5 (25) 5 (45.5) 4 (23.5) 4 (57.1) 1 (20.0) 1 (25.0) 1 (25.0) 2 (20.0) 0 (0) 1 (2.4) PP, no. (%) 0 0 0 0 0 0 0 4 (40.0) 0 (0) 1 (2.4) unknown, no. (%) 0 0 0 0 0 0 0 4 (40.0) 0 (0) 4 (9.5) Ntz treatment characteristics Therapy duration, months, median (range) 28.5 (1–106) 33 (1–106) 16 (1.5–53) 15 (5–51) 62 (25–117) Time after ntz. discontinuation and bx/ax/lumbar puncture, days, median (range) 185 (21–1848) 180.5 (21–617) 259 (22–1848) 188.5 (20–198) 0 (0) Previous treatment Mitoxantrone 1 5 1 3 1 2 0 0 0 0 Interferon beta 0 6 0 4 0 2 1 0 19 0 Glatiramer acetate 2 3 1 2 1 1 1 0 6 0 Fingolimod 4 0 4 0 0 0 0 0 1 0 DMF 2 0 1 0 1 0 0 0 0 0 None 5 1 4 1 1 0 3 0 4 42 Steroidsc 11 2 10 2 2 0 1 0 0 10 PLEXc 6 2 6 1 1 1 0 0 0 0 Abbreviations: ax, autopsy; bx, biopsy; DMF, dimethyl fumarate; Ntz, natalizumab; PLEX, plasma exchange; PP, primary progressive; RR, relapsing-remitting; SP, secondary progressive. a Patients may have more than one demyelinating activity. b Number of lesions analyzed = 1–5. c Relapse therapy within 6 weeks before biopsy/autopsy/lumbar puncture. 2.2 Histology and immunohistochemistryBiopsy and autopsy samples were fixated in formalin and embedded in paraffin. One μm-thick slices were stained with hematoxylin and eosin (H&E), Luxol fast blue/periodic acid Schiff (LFB/PAS) and Bielschowsky silver impregnation. Inflammatory cell infiltrates were detected by immunohistochemistry with an avidin-biotin technique using antibodies specific for CD3 (marker for T cells; clone: CD3-12; AbD Serotec), CD4 (marker for T helper cells; clone: SP35; Zytomed Systems GmbH, Berlin, Germany), CD8 (marker for cytotoxic T cells; clone: L26; Dako DakoCytomation Glostrup, Denmark), CD20 (marker for B cells; clone: L26; Dako), CD138 (marker for plasma cells; clone: MI15; Dako), IL-10 (marker for the anti-inflammatory cytokine interleukin 10; polyclonal; Bioss, Woburn, Massachusetts, USA), CD209 (marker for dendritic cells; clone: 120612; R&D Systems, Minneapolis, MN, USA), MCAM (marker for Th17 cells; clone: EPR3208; Merck Millipore) and KiM1P (marker for macrophages and microglia; clone: KiM1P, University Kiel, Germany). Double fluorescence immunohistochemistry to show MCAM+ T cells was performed using the same primary antibodies and using tyramid amplification for CD3 (Alexa Fluor 555 Tyramid SuperBoost Kit; Invitrogen GmbH, Karlsruhe, Germany). Macrophages and microglia were distinguished according to their morphology. Demyelinating lesion activity was determined using antibodies against myelin basic protein (MBP; polyclonal; Dako) and proteolipid protein (PLP; clone: plpc1; AbD Serotec, Oxford, UK) according to Brück et al. (8) and Kuhlmann et al. (9). Myelin protein degradation products, including the major myelin proteins MBP and PLP, can be detected in the cytoplasm of macrophages during active demyelination, while inactive demyelinated MS lesions show no incorporation of these myelin proteins. Inactive demyelinated biopsy lesions typically still show a substantial number of macrophages, whereas inactive demyelinated autopsy lesions are in general older and present lower macrophage numbers. We cannot exclude with certainty that these biopsies are not representative of the disease process as a whole, but our experience from autopsy studies indicates that these biopsies are typical for the pathological process in general. Histological sections were captured using a digital camera (DP71; Olympus Europa GmbH, Hamburg, Germany) mounted on a light microscope (BX51; Olympus Europa GmbH). Inflammatory cells were quantified at 400x magnification in at least 10 visual fields using an ocular counting grid and are shown as cells/mm2.
2.3 Immune cell phenotyping by fluorescence-activated cell sorting (FACS)Peripheral blood mononuclear cells (PBMCs) were prepared by Ficoll-Hypaque (Biochrom, Berlin, Germany) density centrifugation. CSF samples were centrifuged at 250 g for 10 min at 4°C within 20 min after collection, and the cell pellet was immediately processed by flow cytometry. Cell surface staining was performed using fluorescence labeled anti-CD3, anti-CD4, anti-CD8, anti-CD19, anti-CD45RA, anti-CD45RO and anti-CD138 antibodies (BD Biosciences, Heidelberg, Germany) according to the manufacturer´s instructions. Negative controls included directly labeled isotype-matched irrelevant antibodies (BD Biosciences). After the staining procedure, cells were evaluated by flow cytometry. Cells were measured on a LSR-Fortessa (BD Biosciences) and evaluated by FACS-Diva Software (BD Bioscience).
2.4 Statistical analysisStatistics were calculated using the software GraphPad Prism 5.01 and 6.01. The differences between two groups were analyzed using the Mann-Whitney U test. Group differences of immune cell distribution in the blood versus the CSF were verified by the Wilcoxon matched pairs test. Correlation analyses were done with the Spearman r test. All data are given as median. A value of p < 0.05 was considered significant and is shown by one asterisk. Two asterisks, three asterisks and four asterisks indicate significances of p < 0.01, p < 0.001 and p < 0.0001, respectively.
3 RESULTS 3.1 Pathological, demographic, and clinical characteristicsA total of 24 brain tissue samples taken after natalizumab therapy were available for analysis. Lesion staging showed 17 active demyelinating biopsy areas, 5 inactive demyelinated biopsy areas (2 biopsy specimens contained active demyelinating and inactive demyelinated areas) and 4 inactive demyelinated autopsy lesions of natalizumab-treated MS patients. The disease duration ranged from 1.5 to 23 years (median: 10 years; Table 1). 18 of these patients showed a relapsing-remitting and 6 patients a secondary progressive disease course. The median age at biopsy and autopsy was 38.5 and 41 years, respectively, and more than two-thirds of patients were women. The natalizumab medication was heterogeneous in regard to the number of natalizumab infusions given before biopsy/autopsy, varying between 1 and 101 infusions. In addition, one patient received an oral anti-α4 integrin inhibitor (firategrast) instead of natalizumab infusions. Furthermore, the interval between the last natalizumab infusion and biopsy/death varied between 20 days and more than 5 years. 11 MS biopsies and 10 autopsies with no prior natalizumab therapy were used as controls (Table 1). Lesion staging showed 7 active demyelinating biopsy lesions, 4 inactive demyelinated biopsy lesions, and 10 inactive demyelinated autopsy lesions. The median disease duration at biopsy or autopsy was 7 and 10.5 years, respectively. More patients treated with natalizumab received high-dose corticosteroids (HDCS) and/or plasma exchange before biopsy/autopsy (Table 1). For blood and CSF analyses we included 20 female and 10 male natalizumab-treated MS patients with a median number of 62 natalizumab infusions, ranging between 25 and 117 infusions, and compared them to 42 MS controls (28 female, 14 male; Table 1). The median age of the natalizumab and MS control cohort was 42 years and 37.5 years, respectively. MS controls received HDCS more often than natalizumab-treated patients (Table 1).
3.2 CNS T cell inflammation despite natalizumab therapyT cells were observed in active demyelinating lesions (Figure 1A; MS + Ntz median: 57.6 cells/mm2, MS median: 81.6 cells/mm2) as well as in inactive demyelinated lesions (data not shown) of natalizumab-treated patients, and showed no significant difference as compared to controls. In addition, dissection of the T cell population into CD4+ T helper and CD8+ cytotoxic T cells revealed no significant differences (Figure S1).

T cells are present in MS brain parenchyma despite natalizumab therapy. T cell infiltration was assessed by immunohistochemical staining for CD3 in active demyelinating white matter biopsy lesions. (A) T cell numbers in natalizumab-treated MS patients were compared to MS controls (representative sections, left; quantitative comparison of groups given as median, MS + Ntz: n = 17, MS: n = 7, right; Mann-Whitney U test). (B) T cell numbers with expected natalizumab activity (<3½ months = treatment interruption of less than 3½ months) were compared to T cell numbers where no more natalizumab activity was expected (>3½ months = treatment interruption of more than 3½ months; quantitative comparison of groups given as median, <3½ months: n = 5, >3½ months: n = 12; Mann-Whitney U test)
After discontinuing natalizumab treatment, a reduction in free CD49d receptor binding sites on PBMCs was described for a further 3½ months as compared to levels before the first injection.(10) To determine whether natalizumab activity has an influence on CNS T cell inflammation, T cell numbers in active demyelinating biopsies until 3½ months after the last infusion were compared to T cell numbers with treatment discontinuation longer than 3½ months. No difference in T cell numbers was found when comparing these two groups (Figure 1B; interval between last natalizumab infusion and biopsy or autopsy <3½ months median: 65.6 cells/mm2, >3½ months median: 53.7 cells/mm2).
In experimental autoimmune encephalomyelitis (EAE), an animal model of MS, it was shown that Th17 cells are able to enter the CNS independently of VLA4, which is blocked by natalizumab, suggesting migration via the choroid plexus into the brain parenchyma in a LFA1/ICAM1 dependent manner (11). Along the same lines, natalizumab has been observed to promote differential routes into human CNS by involving PSGL-1 rolling and MCAM-adhesion of TH17 cells (12). To investigate whether natalizumab treatment effects Th17 cell migration, we quantified MCAM+ cells, a proposed marker for Th17 cells (13-15) in the periventricular parenchyma of natalizumab-treated MS patients. We observed single Th17 cells in natalizumab-treated MS patients with no significant difference compared to MS controls (Figure S2).
Taken together, our results suggest that T cell infiltration into the brain parenchyma may occur despite natalizumab therapy.
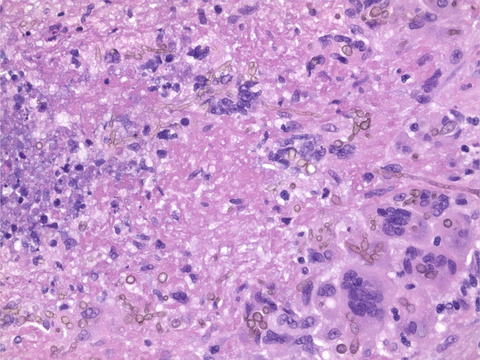
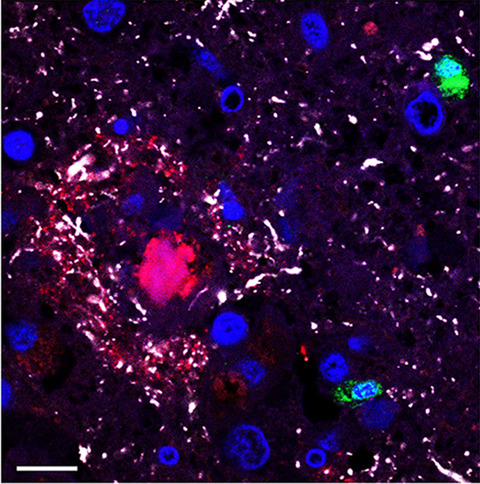
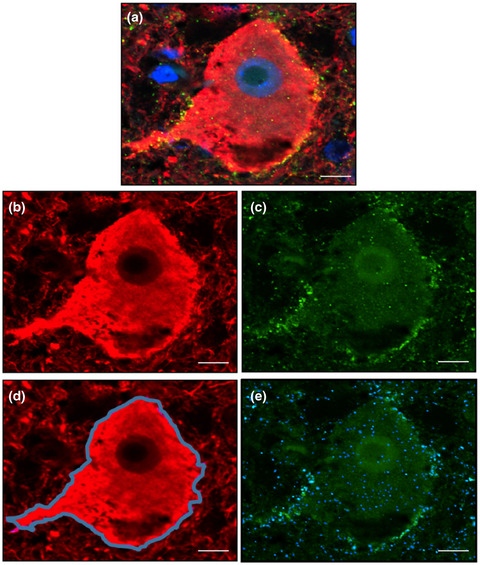
3.3 Plasma cell accumulation in CNS lesions after natalizumab therapyQuantification of plasma cells in the CNS of natalizumab-treated MS patients revealed significantly increased numbers in active demyelinating lesions compared to MS controls (Figure 2A; MS + Ntz median: 7.6 cells/mm2, MS median: 0.4 cells/mm2,p = 0.0156). Also, higher numbers of plasma cells were found in inactive demyelinated biopsy and autopsy lesions (Figure 2B,C) as compared to MS controls, but these differences showed no statistical significance (Figure 2B; MS + Ntz median: 11.6 cells/mm2, MS median: 1.9 cells/mm2,p = 0.14; Figure 2C; MS + Ntz median: 5.5 cells/mm2, MS median: 1.1 cells/mm2,p = 0.1367). In a small number of patients (n = 4 patients with 5 lesion areas), tissue samples were stained for IL-10 and revealed IL-10-positive plasma cells ranging between 7.8% and 68.6% of all plasma cells (Figure S3). By dividing the natalizumab-treated MS patients with active demyelinating lesion activity according to therapy responders (resp.) and non-responders (non-resp.), no obvious difference in plasma cell numbers was evident (Figure 2D), although statistical analyses were not performed due to low numbers of non-responders. As it is known that plasma cell numbers increase with longer disease duration (16), a disease duration-related effect was ruled out by correlation analysis (Figure S4A). Moreover, plasma cell numbers were also not dependent on age (Figure S4B), suggesting a treatment-related effect by natalizumab. Single B cells were observed in natalizumab-treated MS patients with no significant difference to MS controls (data not shown).

Increased plasma cell numbers in MS brain parenchyma after natalizumab therapy. Plasma cell infiltration was assessed by immunohistochemical staining for CD138 (A) in active demyelinating white matter biopsy lesions and in inactive demyelinated white matter (B) biopsy lesions and (C) autopsy lesions (representative sections, black arrowheads indicate individual cells, left; quantitative comparison of groups given as median, MS + Ntz: (A) n = 17 (B) n = 5 (C) n = 4, MS: (A) n = 7 (B) n = 4 (C) n = 10, right). (D) Plasma cell infiltration in patients with active demyelinating white matter biopsy lesions which responded to natalizumab therapy (resp.) were compared to non-responding patients (non-resp.) (representative sections, black arrowheads indicate individual cells, left; quantitative comparison of groups given as median, MS + Ntz resp.: n = 10, MS + Ntz non-resp.: n = 3; (A–C) Mann-Whitney U test)
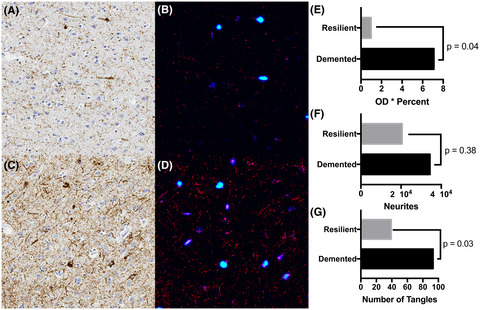
3.4 Reduction in dendritic cells in the CNS with longer natalizumab therapyDendritic cells play an important role in initiation and regulation of immune processes in infections. Natalizumab treatment is associated with the occurrence of the opportunistic infection PML, and we were thus interested in whether dendritic cells were reduced after natalizumab treatment. CD209-positive cells in the CNS of natalizumab-treated patients showed a typical dendritic cell morphology and quantification of dendritic cells revealed no significant difference in active demyelinating lesions (Figure 3A; MS + Ntz median: 2.0 cells/mm2, MS median: 5.9 cells/mm2) and in inactive demyelinated lesions (data not shown) as compared to MS controls. No correlation was found between the number of dendritic cells and the disease duration (Spearman r 0.219; p = 0.94). However, correlation analysis showed a decline in dendritic cells with an increasing number of natalizumab infusions (Figure 3B; Spearman r −0.5402, p = 0.0323), indicating an impaired immune surveillance with longer ongoing natalizumab therapy.

Decreased dendritic cell numbers with longer ongoing natalizumab therapy. (A + B) Dendritic cell infiltration was assessed by immunohistochemical staining for CD209 in active demyelinating white matter biopsy lesions and (B) correlated to the number of natalizumab infusions [(A) quantitative comparison of groups given as median, MS + Ntz: n = 16, MS: n = 7; Mann-Whitney U test; (B) n = 15; Spearman r test]
3.5 No impact on macrophage and microglia numbers in CNS after natalizumab therapyNatalizumab therapy did not alter macrophage and microglia numbers in active demyelinating white matter biopsy lesions (Figure 4).

Natalizumab has no effect on macrophage and microglia numbers in MS brain parenchyma. (A + B) Macrophages and microglia were stained for KiM1P and distinguished according to their morphology in active demyelinating white matter biopsy lesions [(A) representative sections, left; quantitative comparison of groups given as median, (A) macrophages and (B) microglia; MS + Ntz: n = 15, MS: n = 6, right; (A + B) Mann-Whitney U test]
We next analyzed the CSF cell numbers as well as the immune cell composition in the blood and CSF of natalizumab-treated patients and MS controls.
3.6 Reduction in the absolute number of inflammatory cells in the CSF of natalizumab-treated patients, except for memory cytotoxic T cells, B cells, plasmablasts, and plasma cellsNatalizumab therapy is known to reduce the absolute number of inflammatory cells in the CSF (3), and this could also be seen in our cohort (Figure 5A). However, further cell subset analyses revealed that CD8+ cytotoxic T cells and specifically CD8+CD45RO+ memory cytotoxic T cells as well as B cells, plasmablast, and plasma cells were not reduced in natalizumab-treated patients versus MS controls, indicating that these cell subsets were not affected by the treatment (Figure 5B–I).

Reduced absolute number of inflammatory cells in the CSF of natalizumab-treated patients, except for memory cytotoxic T cells, B cells, plasmablast and plasma cells. In the CSF, absolute WBC numbers (A) were quantified after lumbar puncture. The absolute numbers of CD3+ T cells (B), CD4+ T cells (C), CD8+ cytotoxic T cells (D), CD4+CD45RA+ naive and CD4+CD45RO+ memory T cells (E), CD8+CD45RA+ naive and CD8+CD45RO+ memory T cells (F), CD19+CD138− B cells (G), CD19+CD138+ plasmablasts (H) and CD19−CD138+ plasma cells (I) were determined by flow cytometry based on total absolute WBC numbers (quantitative comparison of groups given as median, MS + Ntz: (A, B, D, F left, G, H, I) n = 22, (C, E, F right) n = 21; MS: (A–I) n = 41; (A–I) Mann-Whitney U test)
We then focused in detail on the percentages of inflammatory cell subsets in the blood as well as CSF.
3.7 Increased percentages of memory cytotoxic T cells in CSF of natalizumab-treated patientsWe first focused on T cell inflammation and analyzed the percentage of different T cell subsets of total PBMCs; the results are given as frequencies. Although no changes in T cell subsets were found in peripheral blood after natalizumab treatment compared to controls (Figure S5A–E), within the CSF the frequencies of T cells increased (Figure 6A). Detailed characterization of T cells showed that the frequencies of CD8+ cytotoxic T cells increased, whereas the frequency of CD4+ T cells decreased (Figure 6B,C). The increase in CD8+ cytotoxic T cells could be attributed to an increase in the frequency of memory cytotoxic T cells and a decrease in the frequency of naïve cytotoxic T cells, while no difference in CD4+ naïve and memory T cells was found (Figure 6D,E).

Increased percentage of memory cytotoxic T cells, B cells, plasmablasts and plasma cells in the CSF of MS patients after natalizumab therapy. In the CSF, percentages of CD3+ T cells (A), CD4+ T cells (B), CD8+ cytotoxic T cells (C), CD4+CD45RA+ naive and CD4+CD45RO+ memory T cells (D), CD8+CD45RA+ naive and CD8+CD45RO+ memory T cells (E), CD19+CD138− B cells (F), CD19+CD138+ plasmablasts (G) and CD19−CD138+ plasma cells (H) were analyzed by flow cytometry (quantitative comparison of groups given as median, MS + Ntz: (A, D, E left) n = 22, (B, F) n = 29, (C, G, H) n = 30, (E right) n = 21; MS: (A–D, E left, F, H) n = 42, (E right, G) n = 41; (A–H) Mann-Whitney U test)
3.8 Increased percentages of B cells, plasmablasts, and plasma cells in CSF after natalizumab therapyNext, we analyzed B lineages cells and observed increased frequencies of B cells in the blood, but no effects on plasmablasts and plasma cells were found (Figure
留言 (0)