
記住我




We recruit office desk workers aged between 18 and 67 years from different organizations (i.e. public administration with standard office workplaces) in Germany. Two intervention lines are planned: one live workshop group with and one without reminders. After attending the first workshop participants in the appropriate intervention group will receive reminders via e-mail twice a week. The e-mails remind the participants of the possibilities to be physical active at the work place previously introduced through the workshop. Overall, eight e-mails will be sent until participants answer the second online survey one month after participating in the workshop. We use a randomized allocation of the participants to both groups. As inclusion criteria, we define an age group between 18 and 67 years and the employee council of each institution has to approve the participation. Additionally, participants are asked not to take part in other studies during the time of the workshop intervention. Participants are excluded if they take part in only one workshop or do not fill in the questionnaires (missing answers > 30%) appropriately. All participants will be informed about the content and objectives of our study, they can ask questions, and they can withdraw from the participation at any time. As a prerequisite for participation, participants of our study sign a declaration of consent. A meta-analysis [38] revealed small intervention effects of workplace physical activity interventions (d = 0.21). Based on this assumption, power-analysis (G-Power 3.1) indicated in sum 168 participants for an ANOVA with repeated measures (within-between interaction). Our calculation included f = 0.11, α = 0.05, β = .80, three groups, and three measurements.
Study-aim and procedureOur study aims to examine health-related effects from two slightly different live workshops with office workers. Therefore, we contact health counselors at various companies in Germany. If they are interested in participating in our study, further details will be discussed and the employee council and management level will be involved. If the management approves our study, the health counselors will be interviewed and will help to distribute the information among the employees (i.e. via email). In an email, participation in one of our groups will be clearly explained. The study information and the consent form are attached to this email, with additional contact details of the study supervisors (i.e. regarding upcoming questions). As a prerequisite for participation, these documents must be signed and returned. The participants have the opportunity to choose a suitable date from a list of workshop dates in their company. Each participant receives a link to participate in the online questionnaire as well as an activity diary one week before their first workshop. Additionally, we use accelerometers to objectively measure physical activity during this week. Accelerometers with instructions, activity diaries and an online survey will be sent to all consenting participants for data collection. The instructions explain how to attach the accelerometer to the participant’s thigh and hip. Previous studies have indicated three days are sufficient to observe a stable pattern of physical activity [39]. Not wearing the accelerometer for 3 successive days leads to exclusion of the participant from the study.
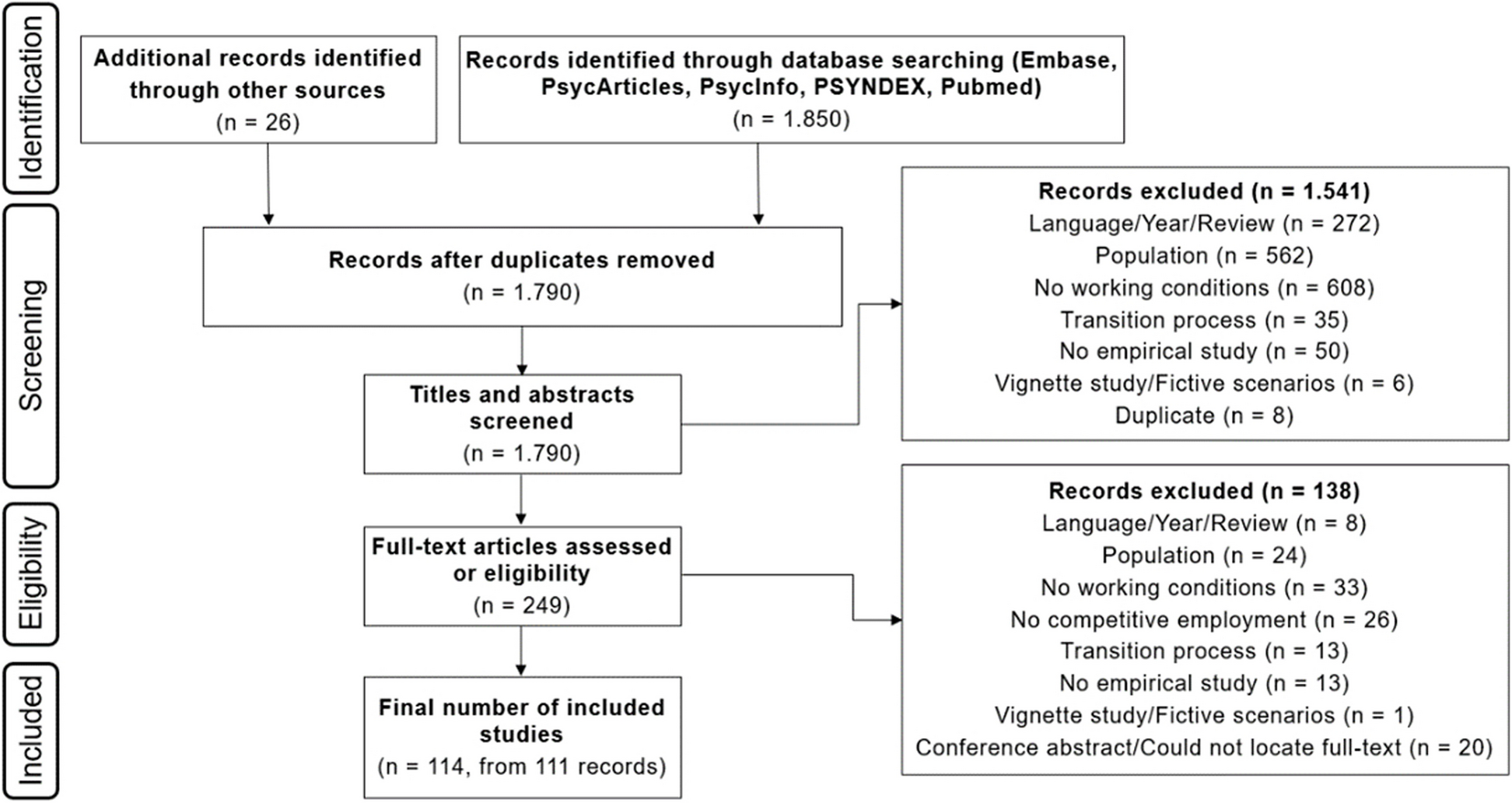
This procedure is repeated one week before the refresher workshop and after six months. We have no blinding of our workshop supervisors and outcome assessors or data analysts. In each group data collection starts one week before the first workshop. The study procedure is presented in Fig. 1.
Fig. 1
Flowchart of the study protocol from contact companies to data analysis (LG = live workshop group). Participants receive a reminder via email
The study lasts about six months for each group. Each workshop and measurement for data collection is promoted by the institutions’ health counselor. Our workshop address three important components for office workers’ health promotion: organizational (i.e. structures, health services), workplace (i.e. equipment, premises), and individual (i.e. health behavior, motivation) components. Details of our intervention are described below. Besides the two interventions groups participants of the control group will receive the pre- and post-study questionnaire.
InterventionThe first workshop lasts about two hours, the refresher workshop only one hour. Each workshop consists of active and passive parts. Table 1 describes the first workshop including active and passive parts. The refresher workshop includes some new activities (see part III in Table 1) as well as an interactive question-answer part. In the latter participants can ask questions about the workshop and further individual strategies, and can discuss adaptations. This concept is used in a live workshop with and without reminders. The reminders are used to retain the acquired contents and knowledge of the first workshop and to give incentives for physical activity.
Table 1 Description of main contents during the workshop; participants were actively (i.e. physically active) or passively involvedThe live workshops take place according to the current hygiene guidelines (i.e. visit https://www.infektionsschutz.de/coronavirus/). These guidelines currently recommend a minimum interpersonal distance of 1.5 m, wearing a personal protective equipment such as a face mask, and good hygiene practices including hand washing etc., (including hand washing for at least 20 s, avoiding touching each other, sneezing into the elbow, etc.). Moreover, further precautionary arrangements are made, for example, smaller size groups, large rooms for sufficient interpersonal distance, regular airing, and disinfection of all tools that are used.
MeasurementsIn the first step, we conduct a structured telephone interview with the health counselor from the company. The respective manual will be attached as supplementary material (S1). The aim is, to explore health offerings, courses, and general attitudes towards employees’ health, health promotion, and programs. Subsequently, small discussion parts of our workshop will be adapted to the company’s framework (i.e. if offices have no height-adjustable desks, we won’t discuss it). Using this approach, we create a crucial prerequisite for multilevel interventions at the workplace: the inclusion of the organization [13].
The subsequently described questionnaires (i.e. Nordic Musculoskeletal Questionnaire, Questionnaire of physical well-being, and Health Action Process Approach) are embedded in one online questionnaire that was built using LimeSurvey, an open-source online survey tool. In compliance with the “Datenschutz Grundverordnung” (DSGVO), we hosted the survey on an internal server from the Charité – Universitätsmedizin Berlin, and participants get an email-link for participation.
Nordic musculoskeletal questionnaire (NMQ)This questionnaire aims to detect musculoskeletal stress in different regions of the body [40]. The NMQ consists of two parts: first, general information about the participant including the individual situation at work, and second, detailed questions about previous and existing physical stress. The latter also examines special regions of the body (i.e. neck, shoulder, lower back). All questions include the duration and frequency of physical stress, especially during the last 12 months and the last seven days. Previous research concluded that the NMQ is sensitive, repeatable, and a useful screening tool [41]. We use this questionnaire in two ways: (i) as a screening tool to adapt the physical activities in our refresher-workshop, and (ii) to record changes in physical stress a few weeks after the workshop.
Questionnaire of physical well-being (FEW-16)The FEW-16 contains some statements about the body, physical capacity, and relaxing. It is a retrospective assessment of the general situation during the last three weeks. Therefore, participants have to indicate the extent to which they agree with the individual statements. The questionnaire contains four scales each includes four items (i.e. stress resistance, ability to enjoy, vitality, and inner peace). Each item is assessed by a six-point Likert scale with a range from zero: “not applicable at all” to five: “fully applicable”. Kolip and Schmidt (1999) reported high internal consistencies (i.e. α = .82 to .92) for the total scale and the subscales and validated the questionnaire with questionnaires on quality of life and functional impairments [42]. Although the FEW-16 contains four scales, in a non-clinical context the physical well-being seems to be one-dimensional [43]. Thus, in our study, we will use the sum-score of all sub-scales. The score ranges from zero to 80 points, in which higher scores represent higher well-being.
Health action process approach (HAPA)The HAPA model (Fig. 2) assumes health behavior as a process with at least two stages: motivation and volition [28, 29]. The first stage includes individuals’ risk perception, outcome expectancies, and task self-efficacy, and results in a formed intention. The latter stage includes planning, execution, and maintenance of health behavior, and leads to actual behavior change. The HAPA model was proven in some empirical studies [29]. The author reported that especially the improvement of action planning and coping planning in patients motivated to increase their physical activity. The questionnaire as well as further information can be received from http://userpage.fu-berlin.de/%7Ehealth/hapa.htm.
Fig. 2
HAPA-model by Schwarzer R. (adapted from Schwarzer, 2008)
The questionnaire contains different subscales (i.e. self-efficacy, planning, intention, outcome expectations, and risk perception). Subscale items are assessed by a four-point Likert scale (i.e. from zero = “not applicable at all” to three: “fully applicable”), except the risk perception with a five-point Likert scale. Scores are computed by adding or averaging the answers over all items.
Physical activity diary (PAD)The physical activity diary is adapted to the German-PAQ-50+ [44], which is a retrospective assessment of one month of daily physical activity. Huy and Schneider (2008) reported acceptable reliability but did not validate the questionnaire as the PAQ-50+ consists of two already validated questionnaires (i.e. YPAS and PASE) [40]. We use the PAQ-50+ in our physical activity diary to assess daily physical activity. Answers are given in hours/week and are added to a sum-score that is multiplied by an appropriate energy score (i.e. MET-value).
Activity trackerPhysical activity is objectively measured by ActivPAL™ (PAL Technologies), which is a validated and reliable accelerometer for activities like sitting, standing, or walking [45, 46]. Especially in sedentary behavior, the ActivPAL™ is a precise and sensitive measurement tool [47]. The sensor is attached to the right thigh and measures not only the number of steps but also various activity patterns. In this study, the measurement is performed over seven consecutive days to examine the average physical activity and to have a comparative value to the PAD.
StatisticsAll data are processed to enhance quality; for example, in case of missing data, we conduct a missing value analysis (MVA) with a subsequent imputation procedure. Outliers are checked manually. Then, it is planned to perform analyses for repeated measurements of physical wellbeing, HAPA subscales, and the results from the physical activity diary. Results from the Nordic Musculoskeletal Questionnaire are analyzed descriptively. For all analyses, the significance level is set to 0.05.
Monitoring and ethicsThere will be no data monitoring committee. However, data will be regularly monitored (i.e. following each workshop) by the principal investigators. There is no external funding for this study and therefore the principal investigators have no financial or other competing interests. Adverse events during the workshops or within data collection will be logged and reported. The study is approved by the ethics committee of Charité Universitätsmedizin Berlin (No.: EA2/185/19). We have to point out that our ethics approval does not yet cover the implementation of reminders. This aspect is currently being submitted in a supplementary application. We assume that this aspect is ethically acceptable and that a corresponding positive vote can be handed in later. Other protocol amendments are not planned. In case an adjustment to the protocol is necessary, this will be indicated in the subsequent report of our results. By publishing this study protocol in advance as well as by using a study registration, all subsequent changes are traceable. Only the principal investigators of this study will have access to the final datasets. All data will be encoded and stored electronically on a password-protected external drive. All identifiable data (i.e. completed questionnaires) are secured as a single version in lockable cabinets that are in lockable rooms.
Only analyses based on aggregated data (n > 15) will be released back to the organization to ensure the anonymity of participants. The invitation to participate in the study will state that participation is voluntary and no negative consequences will impact those that choose not to participate. The overall study results and circumstances will be made available to all individuals irrespective of their group allocation.
留言 (0)