
記住我


Between February 2014 and June 2016, 287 patients at our hospital underwent a combination strategy of therapeutic TACE and RFA to treat HCC. The diagnosis of HCC was made according to the diagnostic criteria used by the European Association for the Study of the Liver [17]. These diagnostic criteria are defined as either two imaging techniques showing typical features of HCC, positive findings on one imaging study together with an α-fetoprotein level of more than 400 ng/mL, or a histologic diagnosis of HCC. All patients signed an informed consent and gave permission to use their clinical data for our research. Our research protocol conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki and was approved by our Institutional Review Board.
According the reference, segments II, IVa, VII, and VIII of the hepatic tumors within 5.0 cm from the root of the main hepatic vein were defined as tumors adjacent to the second hepatic hilus [18]. In this research, we defined the “tumors adjacent to the second hepatic hilus” as the hepatic tumors within 1.0 cm from the main hepatic vein. All patients having a single lesion (1 nodule, ≤ 50 mm) or multiple lesions (up to 3 nodules, ≤ 30 mm each) of the liver and at least one lesion adjacent to the second hepatic hilus (Fig. 1) were included in this study. Patients with extrahepatic metastasis, Child–Pugh class C liver function, and/or uncontrollable ascites were excluded. Based on the previous research of advanced HCC with portal vein tumor thrombosis (PVTT) [19, 20], patients with portal vein thrombosis were also excluded.
Fig. 1
Illustration of the first and second hepatic hilus
Of the 287 patients, 17 patients complicit with the inclusion criteria were included in this study (16 males and 1 female; mean age of 57 years; age range of 33–78 years).
Before treatment, all of the patients underwent a routine physical examination, laboratory testing, and radiologic imaging studies. Imaging studies including a chest CT and a contrast-enhanced abdominal CT scan, or epigastric magnetic resonance imaging were performed within the 2 weeks before TACE.
TACE procedureThe combined TACE and RFA procedures were performed on an inpatient basis in all tumors. Two interventional radiologists (each one who have over 15 years of experience in interventional radiology procedures) performed the combined TACE and RFA procedures.
TACE was performed with a 5 French RH catheter (Cook, Bloomington, Ind), a Cobra catheter (Cook), or a microcatheter (Progreat, Terumo, Tokyo, Japan) being inserted as carefully as possible through the lobar, segmental, or subsegmental arteries, depending on both the tumor location and the hepatic functional reserve of the patient. To start, an emulsion of 2–12 ml of lipiodol (Lipiodol, Guerbet, Aulnay-Sous-Bois, France), 60–90 mg of cisplatin, and 20–40 mg of doxorubicin hydrochloride was injected into the feeding artery. The dosage of lipiodol, cisplatin, and doxorubicin was based on tumor size and vascularity, the presence or absence of an arterioportal shunt, and underlying liver function. Once the emulsion injection was complete, gelatin sponge particles (300–500 µm) mixed with contrast medium were administered into the feeding arteries until stoppage of arterial flow was achieved.
RFA procedureSubsequent RFA was performed as soon as possible following TACE. All 17 patients underwent RFA within the 7 days (3–7 days) proceeding TACE.
RFA was performed percutaneously under CT guidance. A commercially available RFA system (RITA 1500X RF generator, RITA Medical Systems, California) and standard technique were used in this study. All patients were in a supine position while under general anesthesia, and grounding was achieved by attaching two pads to the patient’s thighs. The patients’ heart rate, blood pressure, and oxygen saturation were monitored during the procedure. A preprocedural CT scan of the target area was obtained and all lesions were localized with CT images (Fig. 2A). After confirming the path of the needle with imaging, the RF needles were inserted into the tumor with CT guidance and the electrode was advanced through the catheter. The appropriate RF energy level was achieved by activating the generator, and the average temperature was maintained at 100 °C. First, the electrodes were advanced by 2 cm, and then the electrode needles were advanced and gradually unfolded to 3, 4, or 5 cm until the electrodes crossed the tumor boundary in the target range for ablation. For each intermediate step, RF energy was delivered for 5 min, and in the final step, 7 to 10 min of RF energy was provided. The ablation target range was intended to cover the entirety of the tumor as well as ≥ 5 mm of the surrounding tissue, depending on the adjacent vessels or bile duct. During ablation, the temperature was monitored with a thermocouple in the electrode. To prevent bleeding and tumor seeding, when withdrawing the RFA electrode, we routinely performed tissue ablation of the electrode path in all patients when completing the first ablation. If necessary, the electrode was then moved to a second predetermined location and the electrode tines were reinserted to overlap the ablation procedure. The patients did not receive a preventive antibiotic before or after the RFA procedure.
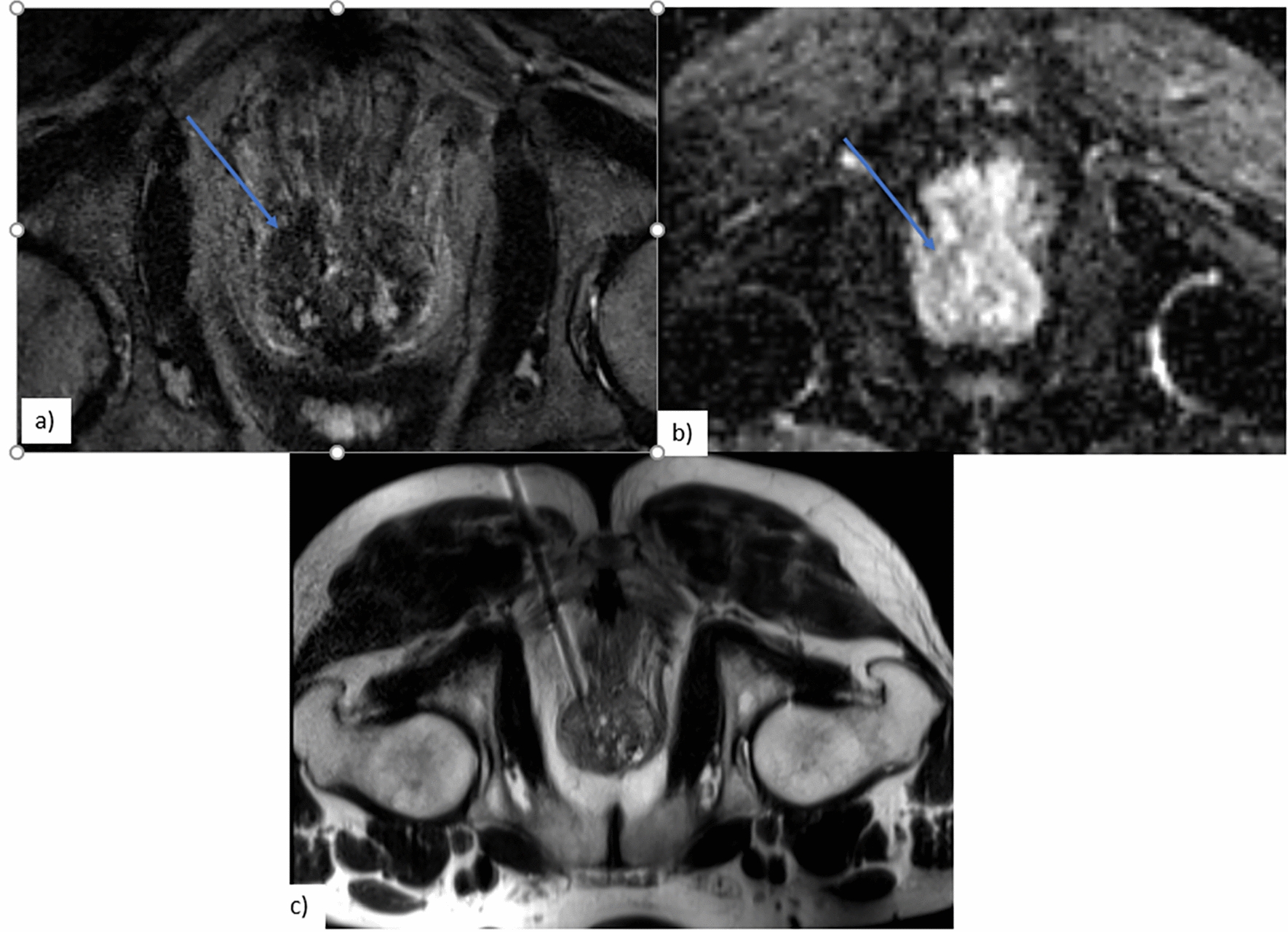
Fig. 2
A 60-year-old man with a 47 mm HCC tumor who underwent combination TACE and RFA treatment. A Five days after the TACE procedure, a CT scan was obtained before the RFA procedure. The scan showed a good iodine deposition in the tumor. B During the 1-month follow-up, the contrast-enhanced CT scan showed a decrease in tumor size. C An enhanced MR image 3 months post treatment showed that there was no tumor survival or vascular injury around the tumor. D 27 months post procedure, the MR image showed a maintained decrease in tumor size and no tumor recurrence
Follow-upThe follow-up was performed on an outpatient basis by three interventional radiologists. The patients were followed up about 1 month after treatment to evaluate the effect by enhanced CT or MRI and laboratory tests measuring tumor markers such as α-fetoprotein. After two consecutive months without progression or recurrence, the follow-up protocols changed into a routine physical examination, laboratory tests measuring tumor markers such as α-fetoprotein every month, and three-phase contrast-enhanced CT or MRI studies every 3–4 months (Fig. 2B–D). We use the mRECIST criteria to evaluate efficacy [21]. Complete response (CR) was determined as complete ablation. Complete ablation was defined as that enhanced CT or MRI scan showed no enhancement of tumor ablation lesions in arterial phase, suggesting complete necrosis of tumor. Primary therapeutic success was defined as achieving a complete ablation of the target tumor. Local tumor progression was defined as the appearance of tumor foci at the edge of the ablation zone after at least one contrast-enhanced follow-up study used imaging standards to record sufficient ablation of the target tumor and the surrounding ablation margin and lack of viable tissue. Distant recurrence was defined as the presentation of new tumors in the untreated portions of the liver or in extrahepatic regions. Follow-up was terminated either at the time of the patient’s death or with the last telephone call through June 1, 2018.
The therapeutic strategy for recurrent tumors was decided using both liver function and tumor backgrounds. RFA should be chosen as the first-line treatment for liver tumors when possible. Combination TACE and RFA therapy or TACE alone is a good choice for treating intrahepatic tumors based on tumor diameter and liver function. If a patient’s Child–Pugh score is over 9 and liver transplantation is impossible, we would recommend palliative care.
ComplicationsComplications were estimated based on previously described guidelines for imaging-guided ablation [20]. A major complication was defined as an event that caused substantial morbidity and/or disability, that necessitated an increased level of care, or that required hospital admission or a substantially lengthened hospital stay. All other complications were defined as minor.
Statistical analysisOverall survival rates were estimated according to the Kaplan–Meier method. All statistical analyses were performed by SPSS software, version 22.0 (SPSS, Chicago, Ill).
留言 (0)