
記住我
Inferior vena cava (IVC) thrombosis is a rare complication of blunt abdominal trauma. Abdominal trauma is associated with severe liver injuries, classified as grade 3 or higher by the American Association for the Surgery of Trauma (AAST)1 (Fig. S1). Although the mechanism of IVC thrombus formation has been previously discussed,2-4 it has not been completely elucidated. We present two cases of patients with mild liver injury that resulted in IVC thrombosis and discuss published findings concerning the reported causes of thrombotic complications.
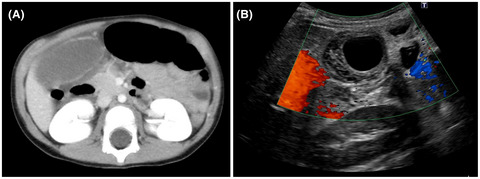
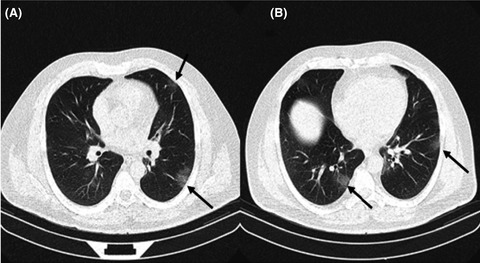
Case reportCase 1 was a 25-year-old woman receiving oral contraceptives for treating dysmenorrhea. The patient was injured in a motorcycle accident and was admitted to our hospital because of abdominal pain. Her vital signs were as follows: Glasgow Coma Scale score, 15; arterial blood pressure, 106/82 mmHg; heart rate, 88 b.p.m.; and oxygen saturation, 97%. The initial blood test results were as follows: hemoglobin level, 16.7 g/dL; platelet count, 221,000/mm3; prothrombin time, 11.7 s; activated partial thromboplastin time (APTT), 21.4 s; aspartate transaminase level, 398 IU/L; and alanine transaminase level, 349 IU/L. The contrast-enhanced computed tomography (CT) findings revealed hepatic contusion of the sixth segment based on Couinaud’s classification, and classified as grade 1 according to the AAST classification.1 No other traumas were detected. The patient was treated conservatively and started walking the day after the injury to prevent thrombosis. Anticoagulants were not provided because of concerns regarding bleeding complications after trauma. During hospitalization, the patient was followed-up with coagulation tests, which showed an upward trend. The contrast-enhanced CT findings at 1 week after the injury revealed thrombus formation with a maximum diameter of 0.6 cm and a length of 0.2 cm (Fig. 1). During this time, the blood coagulation factor was on the rise. Unfractionated heparin treatment was initiated, and APTT was controlled at 50–60 s. At 2 weeks after the accident, the contrast-enhanced CT findings showed that the thrombus had shrunk, and the patient was discharged after replacing the anticoagulant with oral medication.

Imaging findings of a 25-year-old woman taking oral contraceptives for dysmenorrhea who was injured in a motorcycle accident. A, On day 1 of injury, the contrast-enhanced computed tomography findings showed hepatic contusion of the sixth segment (arrow). B, C, At 1 week after injury, contrast-enhanced computed tomography showed thrombus formation in the inferior vena cava (arrows). The thrombus had a maximum diameter of 0.6 cm.
Case 2 was a 58-year-old man who was injured when he was hit from behind by a motorcycle. His vital signs were as follows: Glasgow Coma Scale score, 14; arterial blood pressure, 118/99 mmHg; heart rate, 88 b.p.m.; and oxygen saturation, 94%. The initial blood test results were as follows: hemoglobin level, 15.4 g/dL; platelet count, 218,000/mm3; prothrombin time, 11.5 s; APTT, 24.3 s; aspartate transaminase level, 526 IU/L; and alanine transaminase level, 545 IU/L. The contrast-enhanced CT findings revealed hepatic contusion of the sixth segment based on Couinaud’s classification, and classified as grade 1 according to the AAST classification. The patient also presented traumatic subarachnoid hemorrhage, facial bone fracture, right hemothorax, and multiple rib fractures. We treated the liver injury conservatively and followed up with contrast-enhanced CT at 1 week after the accident. The findings showed a false aneurysm of the hepatic artery at the liver injury site and a thrombus (maximum diameter, 1.5 cm; length, 6.5 cm) in the IVC (Fig. 2). As in Case 1, the patient started walking early, but was not treated with anticoagulants. The hepatic false aneurysm was treated with arterial embolization after implanting an IVC filter. At 1 week after unfractionated heparin treatment, the contrast-enhanced CT findings showed that the thrombus had shrunk. The patient was discharged after replacing the anticoagulant with oral medication.

Imaging findings of a 58-year-old man injured in a motorcycle collision. A, On day 1 of injury, the contrast-enhanced computed tomography findings showed hepatic contusion of the sixth segment (arrow). B, C, At 1 week after injury, the contrast-enhanced computed tomography findings showed the appearance of a hepatic false aneurysm at the site of liver injury and a thrombus (maximum diameter, 1.5 cm; length 6.5 cm) in the inferior vena cava (arrows).
DiscussionInferior vena cava thrombosis is a severe liver injury complication and has been widely reported. We encountered two cases of IVC thrombosis due to mild liver injury. There are 22 previous reports of IVC thrombosis associated with blunt abdominal trauma. Ten cases2-11 (10/22, 45.4%) were associated with liver injury (Table 1). To our knowledge, all reported liver injuries were considered as severe cases (grade 3 or higher) based on the AAST classification.1 Both of our cases developed IVC thrombosis, despite having mild liver injuries (AAST grade 1). After reviewing published reports, we did not find any similar cases.
Table 1. Summary of published reports of inferior vena cava (IVC) thrombosis complicated by traumatic liver injury First author, year Age (years)/sex Damage morphology AAST OIS Other injury Delay (days) Cause of IVC thrombosis Treatment Campbell,5 1981 21/M Hepatic laceration Ⅳ – 19 Endothelial injury, partial disruption of IVC Anticoagulation Kimoto,2 1998 35/M Hematoma Ⅳ Traumatic subarachnoid hemorrhage 35 Endothelial injury Thrombectomy Fujii,6 2002 40/F Hematoma Ⅴ – 30 Hepatic vein thrombosis Thrombectomy, anticoagulation, antiplatelet therapy Mouaffak,7 2004 19/M Parenchymal Unclear Renal contusion 3 – Anticoagulation Nagata,8 2007 9/F Hematoma Ⅲ − 24 Endothelial injury Anticoagulation Hamamoto,3 2013 32/M Hepatic laceration Ⅴ − 31 Hepatic vein thrombosis Thrombectomy, anticoagulation Kim,9 2014 26/M Hematoma Ⅳ − 15 Endothelial injury, partial disruption of IVC IVC filter, anticoagulation Salloum,10 2016 33/M Hepatic laceration Ⅴ − Admission – Thrombectomy, liver lobectomy Chakroun,4 2017 18/M Parenchymal Ⅴ − Admission Endothelial injury Anticoagulation Kano,11 2017 21/M Parenchymal Ⅴ Lung contusion, renal infarction 4 Endothelial injury Anticoagulation Our case 25/F Parenchymal Ⅰ − 7 Endothelial injury Anticoagulation Our case 58/M Parenchymal Ⅰ Brain injury, lung injury 7 Endothelial injury IVC filter, anticoagulation Abbreviations: AAST, American Association for the Surgery of Trauma; F, female; M, male; OIS, Organ Injury Score; –, not reported.The four primary causes of IVC thrombosis due to blunt abdominal trauma, as discussed in a previous work,9 are as follows: hepatic vein thrombosis extending into the IVC, endothelial injury of the caval wall, caval flow stasis caused by compression with a pericaval or retroperitoneal hematoma, and hypercoagulable and hypofibrinolytic states after major trauma. In cases of severe liver injury, there is a complication of hepatic vein laceration and hepatic vein thrombosis extending into the IVC.3 In addition, in cases of blunt abdominal trauma with severe liver injury, damage to the pericaval or retroperitoneal areas can cause hematoma and congestion of caval flow, which can lead to IVC thrombosis.4 These would be the factors that could cause severe liver injury and further result in IVC thrombosis. Regarding endothelial injury of the caval wall, it is thought to be attributed to partial or total detachment of the vein segment caused by shearing forces and inflammatory endothelial proliferation in the caval wall during the healing process.7 The liver, which is a massive and fixed parenchymal organ, is susceptible to shearing forces.7 In these two cases, IVC thrombosis occurred on the anterior surface of the L4 and L5 vertebrae. As the IVC was in contact with the vertebrae, it would be expected that the IVC might have been damaged by shearing force. Therefore, if there was liver injury, even if it was mild, IVC injury would be still possible due to shearing force that might have occurred.
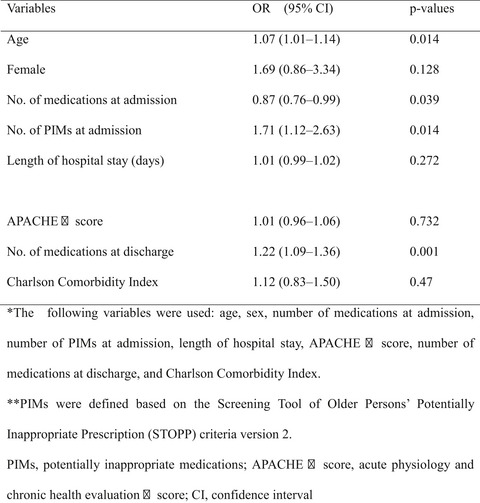
We also consider that the two cases reported here were at risk for venous thrombosis. The risk of venous thrombosis in oral contraceptive users is approximately three times that of nonusers.12 Therefore, oral contraception could have caused a hypercoagulable reaction due to trauma, resulting in thrombosis in Case 1. Following trauma, fibrinolysis and hypercoagulability associated with tissue damage and hypoperfusion can lead to hypercoagulable states.13 Some predisposing factors to venous thrombosis after trauma are leg fracture or head injury with an Abbreviated Injury Scale score of 3 or higher, ventilatory management for more than 3 days, major surgery, age greater than 40 years, and venous injury.14 Because of the threat of severe blood loss, anticoagulant use following injuries remains controversial. Patient 2 sustained a head injury with an Abbreviated Injury Scale score of 3 or higher and was aged more than 40 years; therefore, he had a high risk of developing thrombosis. However, we did not use anticoagulants.
In our cases, the external force at the time of injury was minor and the endothelial injury of the caval wall might not have been serious. However, the combination of thrombogenic factors, such as oral contraceptive and head trauma, could have caused the thrombus.
Our observations suggested that IVC thrombosis due to blunt abdominal trauma should be considered in patients with mild liver injury in the periphery of the IVC and with predisposing factors for thrombus formation. In traumatic injury cases that meet the aforementioned criteria, CT examination for IVC thrombosis should be carried out. Moreover, the elevated blood coagulation factors should be examined up to several days or weeks after injury.
ConclusionTo our knowledge, these are the first two reported cases of IVC thrombosis due to mild hepatic damage. Inferior vena cava thrombosis is a rare complication of liver injury. Although it has been reported in cases of severe liver injury, it can also occur in mild cases. We highlight the need to evaluate the risk factors for IVC thrombosis and undertake regular CT follow-up examinations.
DisclosuresApproval of the research protocol: The ethics committee at our institution approved the publication of this case report.
Informed consent: Consent for publication was obtained from the patient’s family.
Animal studies: N/A.
Conflict of interest: None.
Filename Description ams2691-sup-0001-FigS1.docxWord document, 15.4 KB Fig. S1. American Association for the Surgery of Trauma (AAST) liver injury scale.Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
References
1Moore EE, Cogbill TH, Jurkovich GJ, Shackford SR, Malangoni MA, Champion HR. Organ injury scaling: spleen and liver (1994 revision). J. Trauma 1995; 38: 323– 4. 2Kimoto T, Kohno H, Uchida M, et al. Inferior vena caval thrombosis after traumatic liver injury. HPB. Surg. 1998; 11: 111– 6. 3Hamamoto M, Kobayashi T, Kodama K, Nakamitsu A, Sasaki M, Kuroo Y. Thrombectomy under cardiopulmonary bypass for inferior vena cava thrombosis induced by liver injury. Ann. Vasc. Dis. 2013; 6: 751– 5. 4Chakroun A, Nakhli MS, Kahloul M, Harrathi MA, Naija W. Post traumatic inferior vena cava thrombosis: a case report and review of literature. Int. J. Surg. Case. Rep. 2017; 36: 59– 63. 5Campbell DN, Liechty RD, Rutherford RB. Traumatic thrombosis of the inferior vena cava. J. Trauma 1981; 21: 413– 5. 6Fujii H, Ohashi H, Tsutsumi Y, Onaka M. Open heart surgery for posttraumatic inferior vena caval thrombosis. Eur. J. Cardiothorac. Surg. 2002; 22: 319– 20. 7Mouaffak Y, Mikou M, Benyacob A, et al. Traumatic thrombosis of the inferior vena cava. Ann. Fr. Anesth. Reanim. 2004; 23: 740– 4. 8Nagata K, Yamanouchi T, Shigeru Y, et al. Non-operative management of blunt hepatic trauma in three cases in children. J. Jpn. Soc. Pediatr. Surg. 2007; 43: 928– 32. 9Kim KY, So BJ, Park DE. Management of inferior vena cava thrombosis after blunt liver injury. Korean. J. Hepatobiliary. Pancreat. Surg. 2014; 18: 97– 100. 10Salloum C, Lim C, Hillion ML, Azoulay D. Reconstruction of the inferior vena cava due to blunt hepatic trauma. J. Visc. Surg. 2016; 153: 75– 6. 11Kano K, Hamanaka K, Tanaka H, et al. Massive inferior vena cava thrombosis after liver injury successfully treated with anticoagulation therapy; a case report. JJAAM 2017; 28: 800– 4. 12Peragallo R, Coeytaux R, McBroom AJ, et al. Risk of acute thromboembolic events with oral contraceptive use: a systematic review and meta-analysis. Obstet. Gynecol. 2013; 122: 380– 9. 13Cap A, Hunt B. Acute traumatic coagulopathy. Curr. Opin. Crit. Care 2014; 20: 638– 45. 14Knudson MM, Ikossi DG, Khaw L, Morabito D, Speetzen LS. Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank. Ann. Surg. 2004; 240: 490– 6.
留言 (0)