
記住我
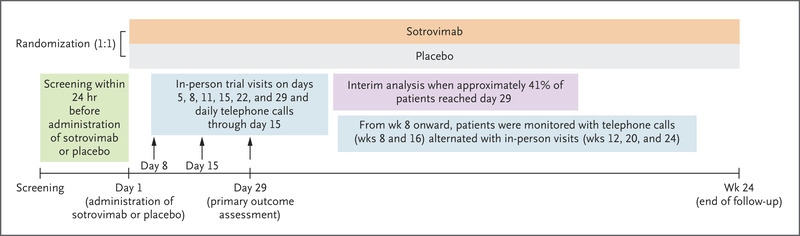


 Figure 1. Screening, Randomization, and Follow-up.
Figure 1. Screening, Randomization, and Follow-up. The diagram represents all enrolled participants 16 years of age or older through the data cutoff date (March 13, 2021). The diagram includes two deaths that occurred after the second dose in human immunodeficiency virus (HIV)–infected participants (one in the BNT162b2 group and one in the placebo group; these deaths were not reported in the Results section of this article because the analysis of HIV-infected participants is being conducted separately). Information on the screening, randomization, and follow-up of the participants 12 to 15 years of age has been reported previously.11
Table 1. Table 1. Demographic Characteristics of the Participants at Baseline.
Table 1. Demographic Characteristics of the Participants at Baseline. Between July 27, 2020, and October 29, 2020, a total of 45,441 participants 16 years of age or older underwent screening, and 44,165 underwent randomization at 152 sites (130 sites in the United States, 1 site in Argentina, 2 sites in Brazil, 4 sites in South Africa, 6 sites in Germany, and 9 sites in Turkey) in the phase 2–3 portion of the trial. Of these participants, 44,060 received at least one dose of BNT162b2 (22,030 participants) or placebo (22,030), and 98% (21,759 in the BNT162b2 group and 21,650 in the placebo group) received the second dose (Figure 1). During the blinded period of the trial, 51% of the participants in each group had 4 to less than 6 months of follow-up after the second dose; 8% of the participants in the BNT162b2 group and 6% of those in the placebo group had 6 months of follow-up or more after the second dose. During the combined blinded and open-label periods, 55% of the participants in the BNT162b2 group had 6 months of follow-up or more after the second dose. A total of 49% of the participants were female, 82% were White, 10% were Black, and 26% were Hispanic or Latinx; the median age was 51 years. A total of 34% of the participants had a body-mass index (the weight in kilograms divided by the square of the height in meters) of 30.0 or more, 21% had at least one underlying medical condition, and 3% had baseline evidence of a previous or current SARS-CoV-2 infection (Table 1 and Table S2).
Between October 15, 2020, and January 12, 2021, a total of 2306 participants 12 to 15 years of age underwent screening, and 2264 underwent randomization at 29 U.S. sites. Of these participants, 2260 received at least one dose of BNT162b2 (1131 participants) or placebo (1129), and 99% (1124 in the BNT162b2 group and 1117 in the placebo group) received the second dose.11 Among participants who received at least one dose of BNT162b2 or placebo, 58% had at least 2 months of follow-up after the second dose, 49% were female, 86% were White, 5% were Black, and 12% were Hispanic or Latinx. Full details of the demographic characteristics of the participants have been reported previously.11
Safety ReactogenicityThe subgroup that was evaluated for reactogenicity in the current report, in which reactions were reported in an electronic diary, included 9839 participants 16 years of age or older. In this subgroup, 8183 participants had been included in the previous analysis, and 1656 were enrolled after the data cutoff for that analysis.9 The reactogenicity profile of BNT162b2 in this expanded subgroup did not differ substantially from that described previously.9 This subgroup included 364 participants who had evidence of previous SARS-CoV-2 infection, 9426 who did not have evidence, and 49 who lacked the data needed to determine previous infection status.
More participants in the BNT162b2 group than in the placebo group reported local reactions, the most common of which was mild-to-moderate pain at the injection site (Fig. S1A). Local reactions were reported with similar frequency among the participants with or without evidence of previous SARS-CoV-2 infection, and the reactions were of similar severity. No local reactions of grade 4 (according to the guidelines of the Center for Biologics Evaluation and Research12) were reported.
More participants in the BNT162b2 group than in the placebo group reported systemic events, the most common of which was fatigue (Fig. S1B). Systemic events were mostly mild to moderate in severity, but there were occasional severe events. Systemic reactogenicity was similar among those with or without evidence of previous SARS-CoV-2 infection, although BNT162b2 recipients with evidence of previous infection reported systemic events more often after receipt of the first dose, and those without evidence reported systemic events more often after receipt of the second dose. For example, 12% of recipients with evidence of previous SARS-CoV-2 infection and 3% of those without evidence reported fever after receipt of the first dose; 8% of those with evidence of previous infection and 15% of those without evidence reported fever after the second dose. The highest temperature reported was a transient fever of higher than 40.0°C on day 2 after the second dose in a BNT162b2 recipient without evidence of previous infection.
Adverse EventsAnalyses of adverse events during the blinded period included 43,847 participants 16 years of age or older (Table S3). Reactogenicity events among the participants who were not in the reactogenicity subgroup were reported as adverse events, which resulted in imbalances between the BNT162b2 group and the placebo group with respect to adverse events (30% vs. 14%), related adverse events (24% vs. 6%), and severe adverse events (1.2% vs. 0.7%). New adverse events attributable to BNT162b2 that were not previously identified in earlier reports included decreased appetite, lethargy, asthenia, malaise, night sweats, and hyperhidrosis. Few participants had serious adverse events or adverse events that led to trial withdrawal. No new serious adverse events were considered by the investigators to be related to BNT162b2 after the data cutoff date of the previous report.9
During the combined blinded and open-label periods, cumulative safety data during follow-up were available through 6 months after the second dose for 12,006 participants who were originally randomly assigned to the BNT162b2 group. No new safety signals relative to the previous report were observed during the longer follow-up period in the current report, which included open-label observation of the original BNT162b2 recipients and placebo recipients who received BNT162b2 after unblinding.9
During the blinded, placebo-controlled period, 15 participants in the BNT162b2 group and 14 in the placebo group died; during the open-label period, 3 participants in the BNT162b2 group and 2 in the original placebo group who received BNT162b2 after unblinding died. None of these deaths were considered to be related to BNT162b2 by the investigators. Causes of death were balanced between BNT162b2 and placebo groups (Table S4).
Safety monitoring will continue according to the protocol for 2 years after the second dose for participants who originally received BNT162b2 and for 18 months after the second BNT162b2 dose for placebo recipients who received BNT162b2 after unblinding.
Efficacy Table 2. Table 2. Vaccine Efficacy against Covid-19 from 7 Days after Receipt of the Second Dose during the Blinded, Placebo-Controlled Follow-up Period.
Table 2. Vaccine Efficacy against Covid-19 from 7 Days after Receipt of the Second Dose during the Blinded, Placebo-Controlled Follow-up Period. Among 42,094 participants 12 years of age or older who could be evaluated and had no evidence of previous SARS-CoV-2 infection, Covid-19 with an onset of 7 days or more after the second dose was observed in 77 vaccine recipients and in 850 placebo recipients up to the data cutoff date (March 13, 2021), corresponding to a vaccine efficacy of 91.3% (95% confidence interval [CI], 89.0 to 93.2) (Table 2). Among 44,486 participants with or without evidence of previous infection who could be evaluated, cases of Covid-19 were observed in 81 vaccine recipients and in 873 placebo recipients, corresponding to a vaccine efficacy of 91.1% (95% CI, 88.8 to 93.0).
Among the participants with evidence of previous SARS-CoV-2 infection based on a positive baseline N-binding antibody test, Covid-19 was observed in 2 vaccine recipients after the first dose and in 7 placebo recipients. Among the participants with evidence of previous SARS-CoV-2 infection based on a positive nucleic acid amplification test at baseline, cases of Covid-19 were observed in 10 vaccine recipients and in 9 placebo recipients (Table S5). Covid-19 was less common among the placebo recipients with positive N-binding antibodies at trial entry (7 of 542 participants, for an incidence of 1.3%) than among those without evidence of infection at trial entry (1015 of 21,521, for an incidence of 4.7%); these findings indicate that previous infection conferred approximately 72.6% protection.
Figure 2. Figure 2. Efficacy of BNT162b2 against Covid-19 after Receipt of the First Dose (Blinded Follow-up Period).
Figure 2. Efficacy of BNT162b2 against Covid-19 after Receipt of the First Dose (Blinded Follow-up Period). The top of the figure shows the cumulative incidence curves for the first occurrence of coronavirus disease 2019 (Covid-19) after receipt of the first dose (efficacy analysis population of participants ≥12 years of age who could be evaluated). Each symbol represents Covid-19 cases starting on a given day, and filled symbols represent severe Covid-19 cases. Because of overlapping dates, some symbols represent more than one case. The inset shows the same data on an enlarged y axis through 21 days. The bottom of the figure shows the time intervals for the first occurrence of Covid-19 in the efficacy analysis population, as well as the surveillance time, which is given as the total time (in 1000 person-years) at risk for the given end point across all participants within each group. The time period for the accrual of Covid-19 cases was from after receipt of the first dose to the end of the surveillance period for the overall row and from the start to the end of the range stated for each time interval. Vaccine efficacy was calculated as 100×(1–IRR), where IRR (incidence rate ratio) is the ratio of the rate (number per 1000 person-years of follow-up) of confirmed cases of Covid-19 in the BNT162b2 group to the corresponding rate in the placebo group. The 95% confidence interval for vaccine efficacy was derived with the use of the Clopper–Pearson method, with adjustment for surveillance time.
Among the participants with or without evidence of previous infection, cases of Covid-19 were observed in 46 vaccine recipients and in 110 placebo recipients from receipt of the first dose up to receipt of the second dose, corresponding to a vaccine efficacy of 58.4% (95% CI, 40.8 to 71.2) (Figure 2). During the interval from the approximate start of observed protection at 11 days after receipt of the first dose up to receipt of the second dose, vaccine efficacy increased to 91.7% (95% CI, 79.6 to 97.4). From its peak after the second dose, observed vaccine efficacy declined. From 7 days to less than 2 months after the second dose, vaccine efficacy was 96.2% (95% CI, 93.3 to 98.1); from 2 months to less than 4 months after the second dose, vaccine efficacy was 90.1% (95% CI, 86.6 to 92.9); and from 4 months after the second dose to the data cutoff date, vaccine efficacy was 83.7% (95% CI, 74.7 to 89.9).
Table 3. Table 3. Vaccine Efficacy against Covid-19 up to 7 Days after Receipt of the Second Dose among Participants without Evidence of Infection.
Table 3. Vaccine Efficacy against Covid-19 up to 7 Days after Receipt of the Second Dose among Participants without Evidence of Infection. Severe Covid-19, as defined by the Food and Drug Administration,13 with an onset after receipt of the first dose occurred in 31 participants, of whom 30 were placebo recipients; this finding corresponds with a vaccine efficacy of 96.7% (95% CI, 80.3 to 99.9) against severe Covid-19 (Figure 2 and Table S6). Although the trial was not powered to definitively assess efficacy according to subgroup, supplemental analyses indicated that vaccine efficacy after the second dose in subgroups defined according to age, sex, race, ethnic group, presence or absence of coexisting medical conditions, and country was generally consistent with that observed in the overall population (Table 3 and Table S7).
Given the concern about the SARS-CoV-2 B.1.351 (or beta) variant, which appears to be neutralized less efficiently by BNT162b2-immune sera than many other lineages,14 whole-viral-genome sequencing was performed on midturbinate samples from Covid-19 cases observed in South Africa, where this lineage was prevalent. Nine cases of Covid-19 were observed in South African participants without evidence of previous SARS-CoV-2 infection, all of whom were placebo recipients; this finding corresponds with a vaccine efficacy of 100% (95% CI, 53.5 to 100) (Table 3). Midturbinate specimens from 8 of 9 cases contained sufficient viral RNA for whole-genome sequencing. All viral genomes were the beta variant (Global Initiative on Sharing All Influenza Data accession codes are provided in the Supplementary Appendix).
留言 (0)