
記住我



Pregnant persons are at risk for severe coronavirus disease 2019 (Covid-19), and infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) during pregnancy is associated with increased risks of preterm birth and other adverse maternal and neonatal outcomes.1 Although spontaneous abortion (pregnancy loss occurring at less than 20 weeks of gestation) is a common pregnancy outcome affecting 11 to 22% of recognized pregnancies (see Table S1 in the Supplementary Appendix, available with the full text of this letter at NEJM.org),2-4 data to inform estimates of the risk of spontaneous abortion after receipt of an mRNA Covid-19 vaccine either before conception (30 days before the first day of the last menstrual period through 14 days after) or during pregnancy are limited.
We analyzed data from the Centers for Disease Control and Prevention (CDC) v-safe Covid-19 vaccine pregnancy registry to determine the cumulative risk of spontaneous abortion from 6 to less than 20 weeks of gestation. Participants with a singleton pregnancy who had received at least one dose of an mRNA Covid-19 vaccine either before conception or before 20 weeks of gestation and who did not have a pregnancy loss before 6 weeks of gestation were included in this analysis. Inclusion of pregnant participants at 6 weeks of gestation is consistent with literature estimating the risk of spontaneous abortion in the general population.2-4 Life table methods were used to calculate the cumulative risk of spontaneous abortion according to gestational week, with appropriate left truncation (i.e., with adjustment for gestational age at entry); data were right-censored at the time of the most recent contact for participants with ongoing pregnancies who were not contacted at 20 weeks of gestation or later and at the time of the outcome for participants who reported pregnancy outcomes other than spontaneous abortion (induced abortions or ectopic or molar pregnancies) before 20 weeks of gestation. The cumulative risk of spontaneous abortion was also age-standardized with the use of data on the risk of spontaneous abortion according to maternal age group.3 We conducted a sensitivity analysis to estimate the maximum possible risk of spontaneous abortion, using an extreme assumption that all participants whose most recent contact was during the first trimester (i.e., at less than 14 weeks of gestation) and whom we were unable to reach during the second trimester experienced a spontaneous abortion immediately after the most recent contact (see the Supplementary Appendix for details).
Table 1. Table 1. Risk of Spontaneous Abortion among Participants in the v-safe Covid-19 Vaccine Pregnancy Registry, December 14, 2020, through July 19, 2021.
Table 1. Risk of Spontaneous Abortion among Participants in the v-safe Covid-19 Vaccine Pregnancy Registry, December 14, 2020, through July 19, 2021. A total of 2456 participants who were enrolled in the CDC v-safe Covid-19 pregnancy registry met the inclusion criteria for this study; 2022 participants reported ongoing pregnancies at 20 weeks of gestation, 165 participants reported a spontaneous abortion (154 participants before 14 weeks of gestation), 65 participants with most recent contact during the first trimester could not be reached for second trimester follow-up, 188 participants completed second trimester follow-up before 20 weeks of gestation, and 16 participants reported another pregnancy outcome before 20 weeks (induced abortion or ectopic or molar pregnancy) (Fig. S1). Most participants were 30 years of age or older (77.3%), were non-Hispanic White (78.3%), and worked as health care personnel (88.8%). Slightly more than half the participants (52.7%) had received the BNT162b2 vaccine (Pfizer–BioNTech) (Table S2). The cumulative risk of spontaneous abortion from 6 to less than 20 weeks of gestation was 14.1% (95% confidence interval [CI], 12.1 to 16.1) in the primary analysis (Table 1) and 12.8% (95% CI, 10.8 to 14.8) in an analysis using direct maternal age–standardization to the reference population. The cumulative risk of spontaneous abortion increased with maternal age (Table S3). In the sensitivity analysis, under the extreme assumption that all 65 participants with most recent contact during the first trimester had a spontaneous abortion, the cumulative risk of spontaneous abortion from 6 to less than 20 weeks of gestation was 18.8% (95% CI, 16.6 to 20.9); after age standardization, the cumulative risk was 18.5% (95% CI, 16.1 to 20.8).
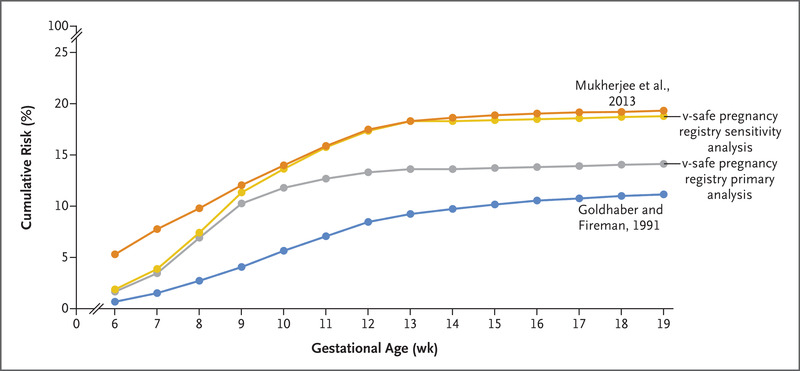
Figure 1. Figure 1. Cumulative Risk of Spontaneous Abortion in the v-safe Covid-19 Vaccine Pregnancy Registry and in Two Historical Cohorts.
Figure 1. Cumulative Risk of Spontaneous Abortion in the v-safe Covid-19 Vaccine Pregnancy Registry and in Two Historical Cohorts. Data from Mukherjee2 were presented as race-specific rates and are provided here for White women to maximize comparability with the v-safe pregnancy registry.
As compared with data from two historical cohorts that represent the lower and upper ranges of spontaneous-abortion risk,2,4 the cumulative risks of spontaneous abortion from our primary and sensitivity analyses were within the expected risk range (Figure 1). Limitations of our study include the lack of a control group of unvaccinated pregnant persons, the homogeneity of the participants in terms of racial and ethnic groups and occupation, the voluntary enrollment of the population, and the use of data reported by the participants themselves, including some data collected retrospectively. Nonetheless, our findings suggest that the risk of spontaneous abortion after mRNA Covid-19 vaccination either before conception or during pregnancy is consistent with the expected risk of spontaneous abortion; these findings add to the accumulating evidence about the safety of mRNA Covid-19 vaccination in pregnancy.5
Lauren H. Zauche, Ph.D., M.S.N.
Bailey Wallace, M.P.H.
Ashley N. Smoots, M.P.H.
Christine K. Olson, M.D., M.P.H.
Titilope Oduyebo, M.D., M.P.H.
Shin Y. Kim, M.P.H.
Emily E. Petersen, M.D.
Jun Ju, M.S.
Jennifer Beauregard, Ph.D., M.P.H.
Centers for Disease Control and Prevention (CDC), Atlanta, GA
Allen J. Wilcox, M.D., Ph.D.
National Institutes of Health, Durham, NC
Charles E. Rose, Ph.D.
Dana M. Meaney-Delman, M.D., M.P.H.
Sascha R. Ellington, Ph.D., M.S.P.H.
CDC, Atlanta, GA
for the CDC v-safe Covid-19 Pregnancy Registry Team
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
The findings and conclusions in this letter are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC). Mention of a product or company name is for identification purposes only and does not constitute endorsement by the CDC or the Food and Drug Administration. The authors do not have any material conflicts of interest.
This letter was published on September 8, 2021, at NEJM.org.
5 References1. Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ 2020;370:m3320-m3320.
2. Mukherjee S, Velez Edwards DR, Baird DD, Savitz DA, Hartmann KE. Risk of miscarriage among black women and white women in a U.S. prospective cohort study. Am J Epidemiol 2013;177:1271-1278.
3. Magnus MC, Wilcox AJ, Morken N-H, Weinberg CR, Håberg SE. Role of maternal age and pregnancy history in risk of miscarriage: prospective register based study. BMJ 2019;364:l869-l869.
4. Goldhaber MK, Fireman BH. The fetal life table revisited: spontaneous abortion rates in three Kaiser Permanente cohorts. Epidemiology 1991;2:33-39.
5. Shimabukuro TT, Kim SY, Myers TR, et al. Preliminary findings of mRNA Covid-19 vaccine safety in pregnant persons. N Engl J Med 2021;384:2273-2282.
留言 (0)