
記住我


Vulvar cancer is a rare malignancy with approximately 6,200 new cases in 2018 [5]. The disease primarily affects post-menopausal women, with the median age at diagnosis of 68 years old [6]. In women older than 60 years, the disease is associated with chronic inflammation and lichen sclerosus [7]. In younger women, the disease is strongly associated with human papillomavirus (HPV) 16 or 18 and vulvar intraepithelial neoplasia (VIN). Although incidence rates have increased in women under 60 years old, high HPV vaccination coverage is expected to reverse the effect on the number of vulvar cancer cases in the vaccinated cohorts [8]. Other risk factors include smoking, HIV, and other genital cancers such as cervical cancer and melanoma.
Women clinically present with symptoms such as pruritus, pain, palpable mass, or bloody discharge. Patients may also be asymptomatic but on exam are noted to have a lesion in the vulva. The lesion may appear as an area of skin thickening or discoloration, raised plaque, ulceration, or palpable lump. A majority of vulvar cancers are diagnosed in the early stages, with 59% of vulvar cancer with localized disease. Approximately 30% of vulvar cancers present with spread to regional lymph nodes and only 6% of vulvar cancers present with distant metastases [6].
PathologySquamous cell carcinoma (SCC) is the most common histologic subtype of vulvar cancer and comprises 70% of cases, with a bimodal distribution affecting women younger than 50 years old and women over 70 years old [9]. SCC arises from epidermal squamous cells and often is associated with vulvar intraepithelial neoplasia (VIN). There are several subtypes of squamous cell carcinoma. The most common is the keratinizing subtype which develops in older women and not associated with HPV. Less common subtypes include basaloid and warty subtypes which are seen in younger women with HPV. Verrucous carcinoma is an uncommon subtype that is slow-growing and correlated with a good prognosis.
The remaining cell types include adenocarcinoma, melanoma, basal cell carcinoma, and sarcoma. Adenocarcinomas most commonly arise from the Bartholin glands at the vaginal introitus. Paget’s disease of the vulva is an adenocarcinoma which mainly affects post-menopausal Caucasian women and originates from vulvar apocrine gland-bearing skin cells. Basal cell carcinoma is generally a slow-growing lesion, primarily located on the labia majora.
Finally, vulvar sarcomas include subtypes such as leiomyosarcomas, epithelioid sarcomas, malignant rhabdoid tumor, and rhabdomyosarcomas. These can be aggressive, have high rates of metastasis, recurrences, and high mortality rate [10]. Unlike other cancers of the vulva, vulvar sarcomas can occur in women of any age, including in childhood.
AnatomyThe vulva is a diamond-shaped soft tissue structure located external to the vagina. The vulva is composed of the following components: labia majora, labia minora, mons pubis, clitoris, vaginal introitus, and the perineal body (Fig. 1). Vulvar malignancies mainly affect the labia, with the labia majora composing about 50% of cases and the labia minora comprising about 20% of cases [11]. The vulva is located in close proximity to the distal vagina, distal urethra, and anal sphincter, which are potential common sites for local invasion.
Fig. 1
Relevant anatomy of the vulva. a Schematic of the vulva anatomy and lymphatic drainage pattern. The vulva is composed of the following components: mons pubis, clitoris, labia majora, labia minora, vaginal introitus, and the perineal body. The pattern of lymphatic drainage from the vulva occurs through a stepwise fashion from the superficial inguinal nodes, to the deep inguinal nodes, and then to the pelvic nodes. b Axial T2-weighted fat-saturated MR image shows the perineal body (asterisk), the urogenital triangle (anterior triangle), and anal triangle (posterior triangle). c Axial T2-weighted MR image shows the clitoris (large arrow), labia minora (small arrow), and labia majora (asterisks). d Axial T2-weighted image shows a superficial inguinal lymph node (yellow arrowhead) located anterolateral to the great saphenous vein (large arrow) and anterior to the femoral vessels (small arrow)
Patterns of spreadVulvar cancer is primarily spread via the lymphatic system. The incidence of inguinofemoral lymph node metastasis is correlated with the depth of stromal invasion, with less than 1% lymph node involvement when the depth of invasion is less than 1 mm, and greater than 8% lymph node involvement when the depth of invasion is more than 1 mm, hence necessitating the need for lymph node dissection [12]. The incidence of deeper iliac chain lymph node metastases is 5%. Hematogenous spread to the lung and bones occur in approximately 4% of patients [13].
The pattern of lymphatic drainage from the vulva occurs through a stepwise fashion from the superficial inguinal nodes (most common), to the deep inguinal nodes, and then to the pelvic nodes. The superficial inguinal nodes are located anterior to the inguinal ligament, the superficial femoral vessels, and the saphenous veins. The deep inguinal nodes are located within the femoral sheath and medial to the common femoral vein. The deep inguinal nodes then drain to the iliac and paraaortic lymph nodes, which are both considered distant metastasis. Metastasis to the contralateral groin or pelvic nodes is rare in the absence of ipsilateral groin metastases. Also, metastasis to the deep inguinal nodes without the involvement of the superficial inguinal nodes has been reported, but this is also rare [14].
ImagingCTCT is useful for detection of lymphadenopathy, determining bladder or rectal invasion and identifying distant metastases, including pulmonary and bony metastases. In addition, CT is used in planning radiation treatment. However, a limitation of CT is its inability to determine local tumor staging due to low soft tissue contrast resolution. Even with contrast-enhanced CT, the vulva may not be well delineated.
MRIThe benefits of MRI imaging include having superior contrast resolution and soft tissue delineation of the primary vulvar tumor as well as being the most sensitive modality for detecting lymph node involvement. MRI is the study of choice for local invasion and treatment response. Small field-of-view images of the pelvis allow for improved anatomy detail and tumor delineation, whereas large field-of-view images offer better detection of lymphadenopathy and bony metastasis. In a 2002 study, Hawnaur et al. determined that MRI had a sensitivity of 89% and specificity of 91% when determining the presence of metastatic lymphadenopathy [15]. In a 2010 retrospective study, Kataoka determined that contrast-enhanced MRI was useful in improving the accuracy of vulvar cancer staging in 85% of a cohort of 20 patients who underwent MRI before surgery [16].
PET-CTPET-CT is useful with radiation therapy planning and as a supplementary imaging tool to lymphatic mapping and sentinel lymph node dissection [17]. In addition, PET-CT is helpful with assessing response to neoadjuvant treatment before surgery and is useful for determining prognosis and patient management. In a 2016 study, Robertson et al. determined that a clinician’s prognostic impression changed in half of the cases following information found on PET-CT. The imaging results helped determine management in 36% of cases, including opting for additional biopsy or treatment in lieu of watchful waiting [18]. On PET-CT, the primary vulvar lesion and the involved lymph nodes will demonstrate FDG avidity.
PET-CT may help detect involved regional hypermetabolic lymph nodes and distant metastases. However, PET-CT has limited value in detecting lymph node metastases less than 5 mm and necrotic lymph nodes. Furthermore, inflammatory lymph nodes can be false-positive on PET-CT [19].
PET-MRIMore recent technology of PET-MRI combines the diagnostic advantages of detailed high-resolution anatomic information from MR with the metabolic information from PET. In a 2018 study comprising a cohort of seventy-one women with gynecologic cancers, Sawicki et al. determined that PET-MRI correctly identified 100% of vulvar cancer recurrences and 84% vaginal cancer recurrences compared to MRI alone [20]. PET-MRI was able to recognize more pelvic recurrences and distant metastases compared to MRI alone.
A potential limitation of fused PET-MRI would be misregistration that can occur between the independently acquired PET and MRI studies. However, newer integrated PET-MRI systems allow for simultaneous acquisition of PET and MRI data, which decreases this.
FIGO classifications and imaging featuresFIGO stage 1FIGO stage 1 vulvar cancers are confined to the vulva or perineum and do not exhibit lymph node involvement or invasion of adjacent structures [21] (Fig. 2). FIGO stage 1A tumor is smaller than 2 cm and with less than 1 mm stromal invasion (T1a). FIGO stage 1B tumor has grown larger than 2 cm or with greater than 1 mm stromal invasion (T1b). On CT, FIGO stage 1 vulvar lesions may appear as vulvar thickening. On MRI, vulvar lesions appear to be T1 hypo-isotense and T2 iso-hyperintense and demonstrate contrast enhancement.
Fig. 2
46-year-old woman with FIGO stage 1 vulvar adenoid cystic carcinoma of the left Bartholin gland. Axial PET-CT shows an intensely FDG-avid soft tissue mass (arrow). There was no evidence of lymphadenopathy or distant metastases (not shown). The pathologic staging was pT1b N0 M0. The mass was excised and the patient subsequently received radiation therapy with chemosensitization
FIGO stage 2FIGO stage 2 tumors can be any size and have partial invasion of adjacent structures including involvement of lower 1/3 urethra, lower 1/3 of vagina, or anus (T2), without metastatic nodal involvement (Fig. 3). MRI is the preferred modality to evaluate for extension of the primary vulvar lesion in locally advanced vulvar cancers. The architecture of the adjacent organs such as the urethra, vagina, and anal sphincter will be disrupted, and the involved portions will demonstrate contrast enhancement. Large necrotic tumors may demonstrate areas of marked T2 hyperintensity. For tumors larger than 2 cm or stage T1 and above, CT or PET-CT may be performed to evaluate for distant metastasis [22].
Fig. 3
69-year-old woman with FIGO stage 2 squamous cell carcinoma of the vulva. a Axial T1-weighted fat saturation with contrast MR image of the pelvis at the level of the vaginal introitus demonstrates irregular thickening in the right labia (arrow). b Sagittal T1-weighted fat-saturated MR image with contrast demonstrates enhancing soft tissue surrounding the distal urethra (arrow), a feature of FIGO 2 stage tumor. Cystoscopy confirmed urethral involvement by tumor with meatal stenosis
FIGO stage 3The hallmark of FIGO stage 3 vulvar cancers is lymph node involvement without distant metastases (Fig. 4). The tumor may be confined to the vulva (T1) or may extend into other structures including the lower urethra, lower vagina, or anus (T2). FIGO stage 3A vulvar cancer involves one inguinofemoral lymph node greater than 5 mm (N1) or it may involve 1 or 2 inguinofemoral lymph nodes less than 5 mm (N1). FIGO stage 3B vulvar cancer involves greater than 3 lymph nodes less than 5 mm (N2a) or the cancer involves 2 or more inguinofemoral lymph nodes greater than 5 mm (N2b). FIGO stage 3C vulvar cancers demonstrate presence of lymphadenopathy with extracapsular spread (N2c), generally pathologically determined. On MRI, metastatic nodal involvement appears to have characteristics such as irregular, rounded, spiculated morphology, short-axis diameter size greater than 10 mm, internal necrosis, loss of fatty hilum, and diffusion-weighted positivity [15]. Inguinal lymphadenopathy can be assessed on large field-of-view post-contrast T1-weighted images.
Fig. 4
75-year-old woman with FIGO stage 3 vulvar cancer who presented with vaginal spotting. a,b Axial PET-CT demonstrates an intensely FDG-avid left vulvar mass (arrow in a) with extension to the right lateral vaginal wall (arrow in b). c FDG-avid right inguinal adenopathy is present (circle)
FIGO stage 4FIGO stage 4A vulvar cancers involves fixed or ulcerated inguinofemoral nodes (N3) or invasion of adjacent structures including the upper 2/3 of urethra, upper 2/3 of vagina, bladder, rectum, or pelvic bone (T3). FIGO stage 4B vulvar cancers involve distant pelvic lymph nodes (internal iliac, external iliac, common iliac, or paraaortic lymph nodes) or have distant metastases (M1), most commonly to the lungs (Fig. 5). Again, large field-of-view post-contrast T1-weighted images are also helpful to assess for pelvic adenopathy.
Fig. 5
55-year-old woman with FIGO stage 4B squamous cell carcinoma of the vulva who presented with a malodorous vulvar mass. a Axial contrast-enhanced CT of the pelvis demonstrates a fungating vulvar mass (arrow). b Bulky left external iliac and inguinal lymphadenopathy was present (arrows). c Axial T1-weighted contrast-enhanced and d axial T2-weighted images show decreased size of the enhancing vulvar mass (solid arrow in c) and external iliac (dotted arrow) and inguinal (solid arrow in d) lymph nodes following radiation treatment
TreatmentTreatment options for vulvar cancer involve a combination of surgery, radiation, and chemotherapy depending on the stage of disease. Surgery is the standard primary treatment of vulvar cancer. With early-stage vulvar cancer, surgery alone may be curative. Treatment of FIGO stage 1A tumor is wide excision. For FIGO stage 1B and 2 tumors, the treatment is radical local excision with sentinel lymph node dissection.
For FIGO stage 3 and 4A patients, treatment options include modified radical or radical vulvectomy with inguinal and femoral dissection followed by radiation treatment. With later-stage or non-resectable disease without major morbidities, neoadjuvant chemotherapy is the primary treatment. Consideration can be given for surgical removal of residual disease following chemoradiation. Newer management strategies start with neoadjuvant radiation therapy and/or chemoradiation of the primary lesion.
For stage 4B patients, there is no current standard treatment for advanced vulvar cancer. However, chemotherapy regimens that have been attempted include 5-fluorouracil (5-FU), cisplatin, mitomycin-C, or bleomycin [11]. Addition of palliative radiation may also be an option. Newer agents with targeted approaches toward immune signaling are promising therapies for HPV-driven vulvar malignancies [23].
Survival/prognosisNodal status is the most important factor for survival, with an 86% 5-year survival rate in women who do not have lymph node involvement and 53% 5-year survival rate in women who have lymph node involvement [5].
The survival rate decreases as the FIGO stage increases. The FIGO staging and overall survival at 5 years is as follows: FIGO 1- 78%, FIGO 2- 59%, FIGO 3- 43%, and FIGO 4- 13%. The 5-year survival rate decreases to 19% when distant metastasis is identified [5].
Recurrence rates of vulvar SCC range from 30-50% within the first 2 years. Other prognostic features include tumor size, depth of invasion, and presence of metastatic disease [24].
Post-treatment imagingAccording to the NCCN (National Comprehensive Cancer Network), history and physical examination are recommended every 3 to 6 months for 2 years, followed by every 6 to 12 months for another 3 to 5 years, and then annually. Low-risk disease patients will have a longer follow-up interval whereas high-risk disease patients will have a shorter follow-up interval. Imaging is indicated by suspicious physical examination findings or symptoms of recurrence [25]. The purpose of post-treatment imaging includes assessing complications of treatment and identifying residual or recurrent tumor. A routine imaging surveillance strategy has not yet been established.
ComplicationsPost-treatment changes and complications after radical vulvar surgery include inflammatory reaction, pelvic floor prolapse, and urinary or stool incontinence (Fig. 6). Potential complications of groin lymph node dissection include lymphedema, lymphocele, wound infection or necrosis, hematoma, cellulitis, and hernia formation [26].
Fig. 6
51-year-old woman with FIGO stage 1B squamous cell carcinoma of the vulva status post-excision. a Axial PET-CT image 3 weeks after surgery shows intense linear FDG uptake along the right vulva (arrow). b Axial PET-CT image six months later shows decreased FDG uptake. The previous findings reflect post-treatment inflammation reaction (arrow)
Early complications of radiation therapy include cellulitis, urethritis, vulvar edema, and diarrhea. Radiation-induced bone changes or fractures, myositis, fistula formation, and radiation-induced secondary tumors are late complications of radiation therapy. Fistulae between the bowel, vagina, or bladder can occur.
RecurrenceLocal structures in the perineum serve as common sites of recurrence. Approximately 30% of recurrence can occur in the groin, which is associated with a worse outcome [27]. MRI can help delineate local recurrence whereas PET-CT can detect distant and nodal metastasis, particularly in the inguinal region with a 100% sensitivity and 89% specificity rate for positive inguinal nodes [28] (Fig. 7).
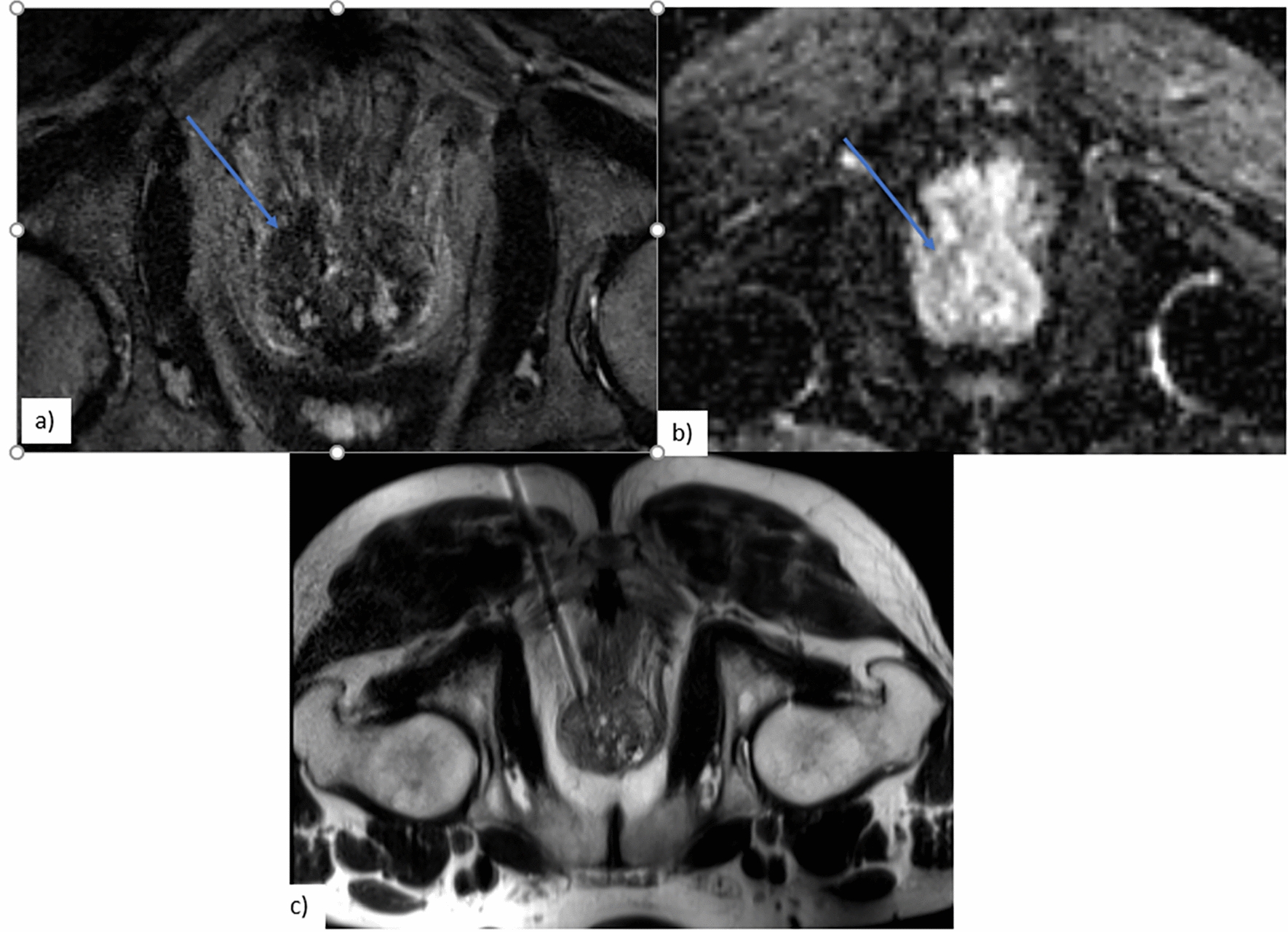
Fig. 7
56-year-old woman with FIGO stage 4A SCC of the vulva status post-hysterectomy, bilateral oophorectomy, and radiation with recurrent disease 6 months later. a Axial T1-weighted contrast-enhanced and b DWI (b = 1000) MR images show a nodule measuring around 1 cm in the right vulva with enhancement and restricted diffusion (arrow). ADC image shows corresponding hypointensity (not shown). c Axial PET-CT image demonstrates soft tissue thickening in the right vulva with focal intense FDG uptake (arrow)
留言 (0)