
記住我


Research ethics board approval and investigational device exemption were obtained to perform a prospective, single-arm, non-blinded feasibility, and safety clinical trial of the PUG technique with comparison to a propensity score-matched retrospective control cohort receiving standard PRG (ClinicalTrials.gov ID NCT03575754). This industry-sponsored first-in-human clinical research trial was conceived by the sponsor (CoapTech, Baltimore, MD); however, all data collection and analyses were performed locally by the authors without sponsor oversight. The writing of all drafts of the manuscript and decision to publish were done by the authors alone. None of the authors have a financial relationship with the sponsor or any other relevant conflicts of interest.
All adults ≥ 18 years of age referred to the interventional radiology department with an indication for gastrostomy tube insertion between October of 2018 and April of 2020 were screened for enrollment in the prospective PUG group. Exclusion criteria included a history of prior gastrostomy tube; BMI < 20 kg/m2 or > 30 kg/m2; untreated esophageal cancer or esophageal stricture; untreated or recently resected head and neck cancer; prior major upper abdominal surgery or suboptimal positioning of the stomach based on any available prior imaging; other esophageal, head and neck, or upper abdominal condition or anatomy considered by the operator to preclude safe insertion of the orogastric balloon; active life-threatening hemorrhage, hematocrit < 0.25, or blood transfusion within the preceding 14 days; temperature > 38 °C, systolic blood pressure < 100 mmHg or > 180 mmHg, or heart rate < 50 BPM or > 100 BPM; contraindication to being placed in proximity to a magnet, such as possessing a pacemaker; pregnant or nursing women; and individuals in which sedation is contraindicated, such as those with bulbar palsy or amyotrophic lateral sclerosis. The decision to pursue gastric feeds as opposed to post-pyloric feeds was made by the referring primary care teams.
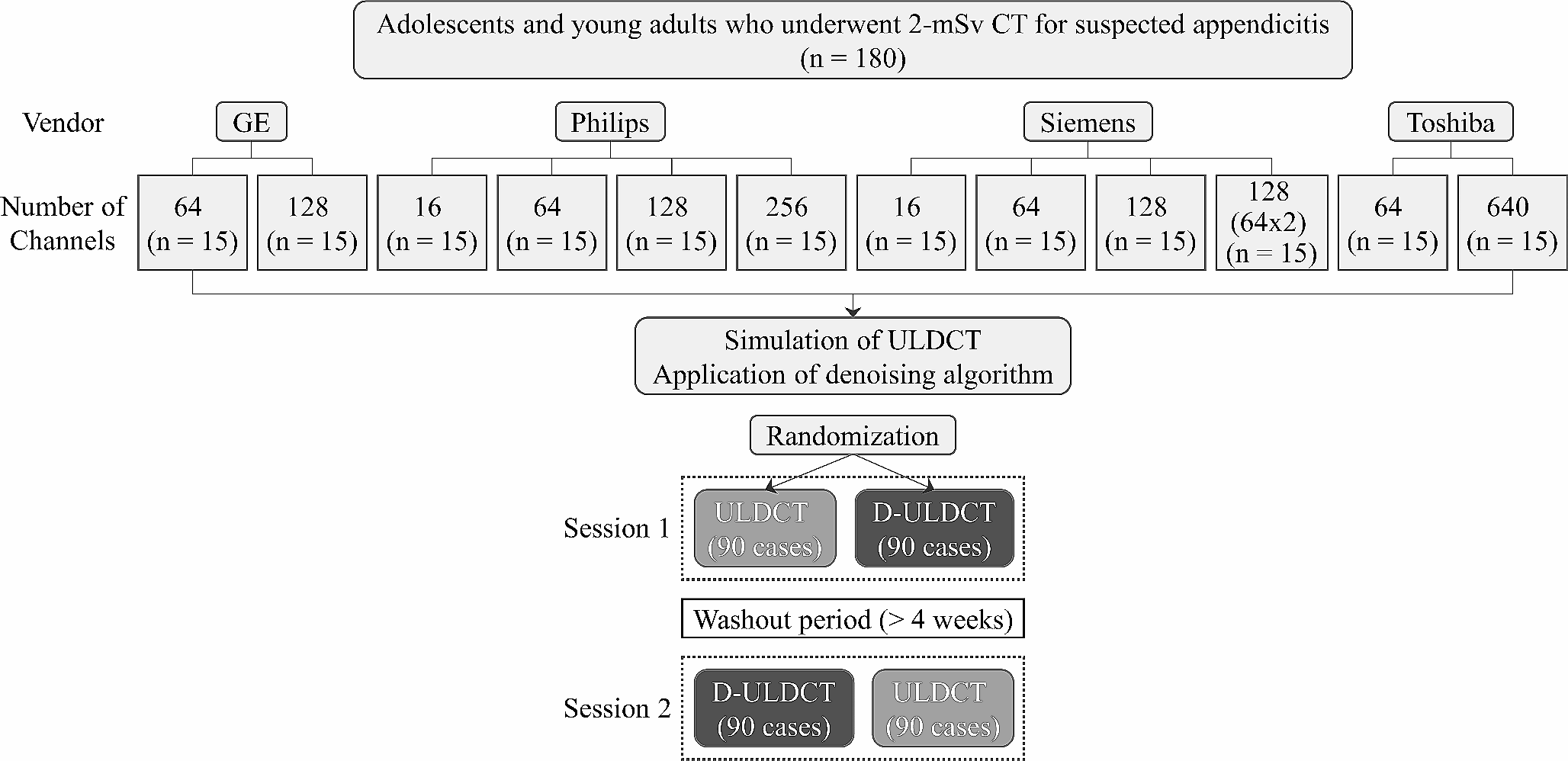
Of 150 consecutive patients screened, on whom exclusion criteria were applied, 25 participants were enrolled for percutaneous ultrasound gastrostomy (Fig. 1). A sample size of 25 was selected to establish the first-in-human early safety and efficacy data for the new technique. The first five participants of this study were previously included in a brief report describing the PUG procedure technique [3]. The current study reports on the full clinical trial with quantitative analysis of the safety and efficacy measures and includes comparison to a matched historical cohort receiving PRG.
Fig. 1
Breakdown of excluded and enrolled individuals. The number of individuals meeting each specific criterion within a category is shown in parentheses. Thirteen individuals met two exclusion criteria simultaneously
Procedural techniqueThe setting for the PUG insertion (bedside vs. IR department) was determined by the patient’s hospital location. PUG procedures were performed bedside within the ICU for all patients located in the ICU, while PUG procedures for all other patients were performed in an angiographic suite. Portable fluoroscopy was not made available for cases performed bedside within the ICU. The PUG procedure has been previously described [3], is summarized below, and is depicted in Video 1. PUG was performed using a Point-of-Care Ultrasound Magnetically Aligned Gastrostomy kit (PUMA-G System, CoapTech LCC, Baltimore, MD), which includes a reusable handheld external magnet, a single-use orogastric balloon catheter with a bar magnet at the tip, and a coil-tipped guidewire. PUG insertions were performed by one of two interventional radiologists with procedure assistance from the scrub nurse and the circulating technologist that are routinely part of IR procedures.
Titrated doses of Fentanyl and Midazolam were used in all procedures to achieve moderate sedation. The oral cavity was anesthetized with topical lidocaine spray and, if not already in place, a nasogastric tube was inserted to insufflate the stomach. The orogastric balloon was inserted through the mouth into the stomach in a non-sterile manner by the interventional radiologist, and the handheld magnet was placed over the epigastrium by the assistant, drawing the balloon catheter against the anterior gastric wall and achieving magnetic gastropexy. For the purposes of this study, if magnetic coaptation was not achieved, fluoroscopy could be used at the operator’s discretion to locate the orogastric balloon within the stomach and aid in magnetic coaptation. If magnetic gastropexy was not achieved at the bedside within the ICU, the procedure would be rescheduled within a fluoroscopic suite. Once magnetic coaptation was achieved, the interventional radiologist scrubbed in to perform the epigastric ultrasound-guided gastrostomy puncture in a sterile fashion. The orogastric balloon was inflated with 20–30 ml of saline by the assistant, allowing it to be visualized with ultrasound through the abdominal wall. Using real-time ultrasound guidance, an 18-gauge needle was used to puncture the balloon through the abdominal wall to create the gastrostomy tract (Fig. 2). The provided guidewire was inserted through the needle and uncoiled in, or through, the balloon. The balloon was deflated by the technologist to mechanically capture the guidewire, allowing the wire to be drawn out of the mouth by the interventional radiologist, leaving a ‘through-and-through’ guidewire from mouth to gastrostomy site. A 20-French bumper style gastrostomy tube (FLOW 20® PUSH PEG, Cook Medical, Bloomington, IN) was then fed through the guidewire using Sacks-Vine per-oral gastrostomy insertion technique [4].
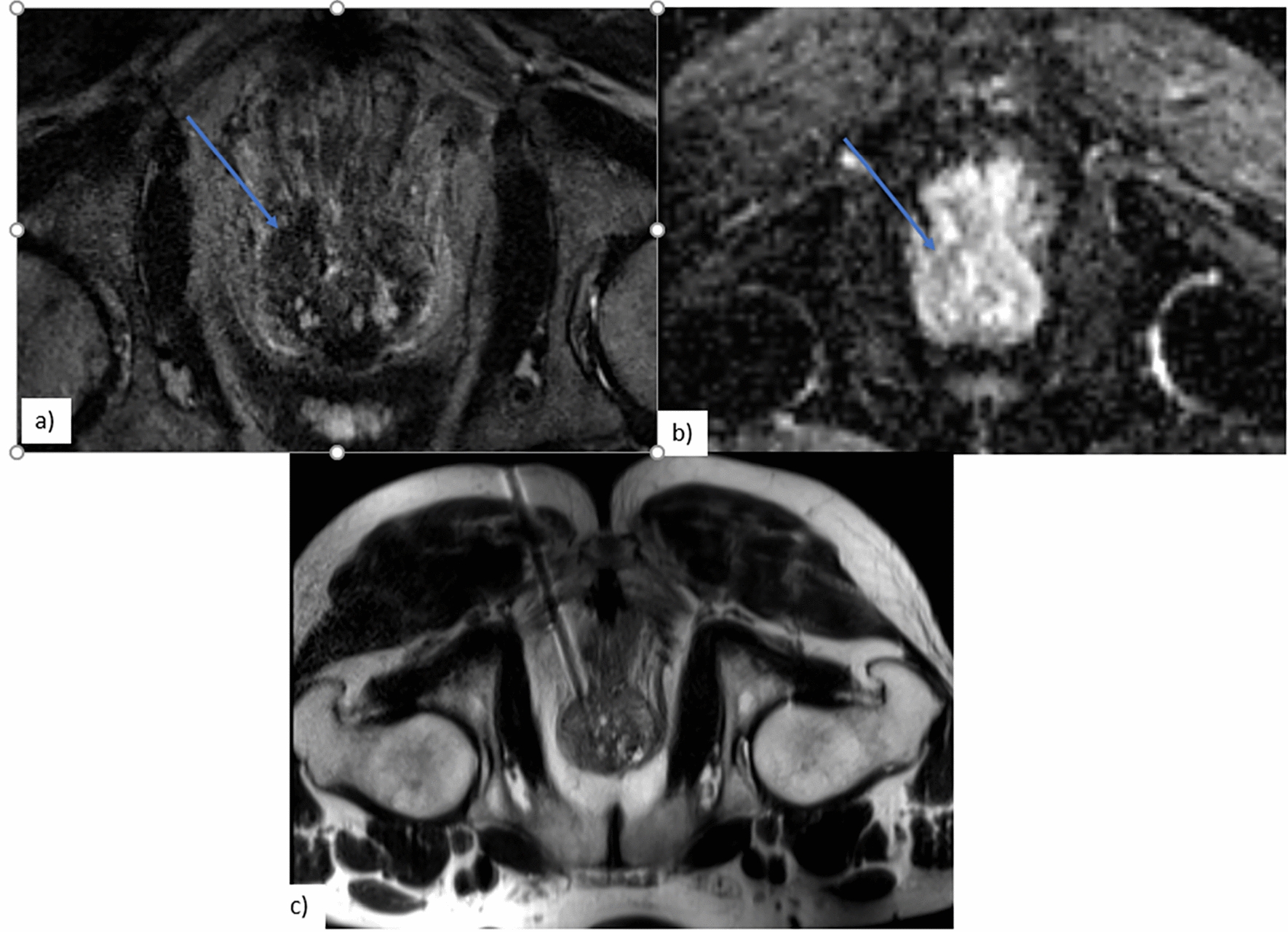
Fig. 2
Transabdominal ultrasound of the inflated orogastric balloon (arrow) within the gastric lumen. The orogastric balloon is being pulled against the anterior gastric wall via magnetic gastropexy. An 18-gauge needle (arrowhead) is advanced through the abdominal wall into the orogastric balloon, creating the gastrostomy tract
Two protocol deviations for the PUG procedure occurred during the study. Firstly, pre-procedural prophylactic Cefazolin 1 g IV was administered commencing with the seventh enrolled individual. Administration of prophylactic antibiotics was added to adhere to recommendations for PEG insertion [5], on the basis that both PEG and PUG require advancement of the gastrostomy tube through the mouth and esophagus, increasing the risk of infection with oral microflora at the gastrostomy site. Conversely, institutional practice does not routinely administer antibiotic prophylaxis for PRG and no consensus exists for its use in SIR guidelines [6]. Second, a reusable Gauss meter (Gauss Meter Model VGM, AlphaLab Inc., Salt Lake City, UT) was incorporated into the PUG procedure starting with the tenth participant to assist with the challenge of locating the orogastric balloon within the stomach without fluoroscopic assistance. This handheld meter measures magnetic force with a small directional detector, which was manipulated over the epigastrium during the insertion of the orogastric balloon catheter to detect the position of the balloon’s magnet within the stomach and assist in magnetic coaptation/gastropexy.
PRG insertions were performed with either 12-French Cope-loop multipurpose catheters in 21/25 cases (84%) (Cook Medical, Bloomington, IN; or Boston Scientific, Marlborough, MA) or with 14-French balloon-retention gastrostomy feeding tubes in 4/25 cases (16%) (Avanos, Alpharetta, GA). The type of PRG tube used was primarily based on operator preference. De novo insertion of PRG tubes larger than 14F was not part of the institutional or regional practice. Conversely, the smallest caliber per-oral PEG tube available within the institute was 20F. Hence, a discrepancy in gastrostomy tube size could not be controlled with the propensity match. Specific indications for gastrostomy insertion in each group are outlined in Table 1. PRG insertions were performed by one of six operators, including the two operators involved in PUG insertion.
Table 1 Indications for gastrostomy tube insertion within the PUG and PRG groupsFollow-upParticipants were maintained NPO with no enteral feeding for 24-h post-insertion. Following the established institutional practice for PRG, all outpatients were admitted post-PUG insertion under the care of the referring service and were discharged by the referring service after nutritional targets were met (typically resulting in a 48-h admission). Clinical follow-up was performed by an interventional radiologist at 48-h and 30-day post-procedure.
OutcomesPrimary outcomes included procedural success (defined by insertion of a gastrostomy tube into the stomach lumen and achievement of target nutrition) and 30-day procedure-related adverse events (defined by the 2017 SIR adverse event classification system for interventional radiology procedures) [7] (Table 2).
Table 2 Society of interventional radiology adverse event classification for interventional radiology procedures [7]Secondary outcomes include sedation requirements (utilization and dose of Fentanyl and Midazolam), hospital length of stay (only for outpatients admitted specifically for gastrostomy tube insertion), and procedural duration.
Duration of PUG insertion was prospectively recorded by an independent technologist within the room. Length of procedure was defined as the time from pre-procedural ultrasound (start of procedure) until the gastrostomy tube was successfully in place. Time to magnetic gastropexy was defined as the time from the start of procedure to magnetic coaptation. Procedural room time for PUG was defined as the time from patient entry to patient egress from the procedural room. Procedural room time for PRG was recorded in the electronic medical record, as for all interventional procedures, commencing with patient entry into the procedure room and terminating when the study was completed by the technologist in the electronic medical record.
Control matchingPotential controls were identified by retrospective chart review of all adult PRG procedures performed at the same center in the nine months prior to the first PUG insertion. The same inclusion and exclusion criteria used for the PUG group were applied to the retrospectively identified cohort receiving PRG. A database of 55 potential institutional controls was generated.
Propensity score matching was performed using ‘R: A language and environment for statistical computing’ [8] employing the statistical package ‘MatchIt: Nonparametric Preprocessing for Parametric Causal Inference’ [9]. Propensity scores were generated for age, sex, and inpatient status, felt to be the covariates most likely to affect selection for PUG versus PRG in a routine clinical setting. The ‘optimal matching’ method was used. Propensity score matching resulted in a well-matched group of twenty-five individuals who received PRG, with similar demographic distribution to the PUG group (Table 3).
Table 3 Demographic information for the PUG treatment group and PRG control groupStatistical analysisStatistical differences in outcomes between the treated and control groups were evaluated with standard t tests for outcomes with continuous variables (e.g., sedative dose) and two proportion z tests for outcomes with categorical variables (e.g., adverse events). To account for the problem of multiple comparisons and control for familywise error, the significance level (alpha) was adjusted where applicable using the Holm–Bonferroni correction method and explicitly stated in the text as a ‘corrected alpha.’ A starting alpha of 0.05 was used. Single comparisons performed on subgroups (e.g., length of stay for outpatients only) use a standard alpha of 0.05. Trends in procedural length throughout the study were tested using the Pearson Product-Moment Correlation method. Margin of error estimations for adverse events referenced in the discussion were performed using standard formulas for sample size determination for two independent variables with dichotomous outcomes.
留言 (0)