
記住我

Sweden has more than 100 health care quality registers that complement government-administered registries by collecting data on disease specific measures (Emilsson et al. 2015). The Swedish national quality register for bipolar disorders (BipoläR) was established in 2004 with the aim of improving the quality of care for BD patients in Sweden (BipoläR 2021). We used data from BipoläR because it contains more detailed information than the Swedish patient register where data is limited to international classification of diseases diagnoses: BipoläR contains information on, e.g., bipolar disorder subtype and psychiatric comorbidities, incident mood episodes managed in outpatient care, education, medication, and body mass index. In June 2016, the register contained more than 55,000 registrations of almost 20,000 unique patients (BipoläR 2021). Participation is voluntary for the clinician as well as the patients. Registering units include both private and public psychiatric outpatient health care units in Sweden (a total of 191 units were active in June 2016).
The quality register contains individualized data on bipolar subtype (BD I, II and NOS) and current comorbid psychiatric conditions according to Diagnostic and Statistical Manual of Mental Disorders-IV, interventions, and outcomes. The diagnoses are made in regular care and diagnostic assessments reflect clinical routine. This means that the use of structured diagnostic instruments varies across participating clinics but the mini-international neuropsychiatric interview is commonly used. During 2019, any form of structured diagnostic instrument had been used in 44% of new registrations in BipoläR. After the baseline registration, information about interventions and outcomes during the last 12 months is collected at annual follow-up examinations. At the annual follow-up, the number of depressive, manic, hypomanic, and mixed episodes are documented based on the patient interview and reviewing the past 12 months medical notes. This information is typically collected by the treating psychiatrist, or nurses trained in the diagnosis and treatment of bipolar disorder, who have access to all clinical data for the patient. Data are entered into a web-based application. Quality control is performed by data type restrictions and boundaries for registered values. Further, completeness and coverage of register data is checked annually. Diagnostic codes have also been benchmarked against medical records. Finally, the validity of the register has been assessed by comparing summary statistics to information in the national patient register and the Swedish prescribed drug register (BipoläR Årsrapport 2021).
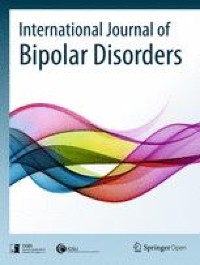
Study population and measuresIn the current study, we included patients diagnosed with BD I, BD II, or BD NOS. At the time of data extraction (June 2016), 19,948 patients were included in BipoläR, of whom 14,616 patients were diagnosed with BD I, BD II, or BD NOS and not excluded due to other missing data (Fig. 1). Of the 14,616 patients, a total of 5618 patients were diagnosed with BD I.
Fig. 1
Flowchart of inclusion and exclusion of study subjects
The following variables were extracted from BipoläR: BD subdiagnoses, psychiatric comorbidity, number of episodes during the past 12 months, current psychotropic drug treatment, age, sex, weight, height, and educational level. We used the most recent register entry for each patient regardless of year of entry.
Dichotomous variables were created for each type of episode that had occurred during the last 12 months prior to the last register entry. Psychiatric comorbidity was extracted both as any type of comorbidity, and as the following specific comorbidities: substance abuse or addiction, anxiety disorders, and personality disorders. Mood stabilizing drugs were in this study categorized as any mood stabilizer (lithium, lamotrigine, valproate, or carbamazepine), lithium, lamotrigine, valproate, and carbamazepine. Second generation antipsychotic drugs (e.g., olanzapine and quetiapine) might also qualify as mood stabilizers (Rybakowski 2018), but were here classified as neuroleptics because they are often used temporary to treat acute episodes and as needed rescue medication.
Items included in BipoläR have been subject to change over the years, some of which affected the choice of outcomes and variables for the present analyses. For example, in 2014 the variable concerning educational level was removed. Educational level is therefore presented for all study populations along with the number of missing data, but is not included in the regression analyses.
The analyses were conducted in two steps: we first analysed the 14,616 patients with BD I, BD II, or BD NOS. Secondly, as evidence for lithium in long-term prevention varies extensively between the subtypes (strongest for BD I) (Severus et al. 2014; Miura et al. 2014), separate analyses of the subsets of patients with BD I, BD II and BD NOS were carried out. The lithium prescription rate—defined as the proportion of bipolar disorder patients being on lithium at the time for annual follow-up—was calculated for each county. The prescription rate for the total population stratified by county is shown in Fig. 2. The same calculation of prescription rate was also made for the three subpopulations BD I, BD II and BD NOS. Further details on the prevalence of lithium use in the 21 Swedish counties and for the three subsets of patients can be found in the supplement.
Fig. 2
County specific lithium prevalences. All BD patients
StatisticsThe primary outcome was any type of mood episode (coded ‘yes’ if at least one episode had occurred during the 12 months preceding the registration). Secondary outcomes were separate counts of depressive, manic, hypomanic, or mixed episode.
Logistic regression analyses conducted with relapse as the dependent variable and county lithium prevalence as the main independent variable were performed in two steps: (1) adjusted for age and sex; (2) also adjusted for psychiatric comorbidity (any type); two-sided testing was used for all analyses and the significance level was set to p < 0.05.
Results are presented with adjusted odds ratios (aOR) for a 10% point increase in lithium use prevalence, 95% confidence intervals (CI), P-values when applicable, and estimated (pseudo) R2-values (Cox–Snell and Nagelkerke) for the different county groups. No problematic multicollinearities were found for the variables age, sex, psychiatric comorbidity (any type) and lithium prescription rate. IBM SPSS version 24 was used for all analyses.
It is possible that minor changes of lithium prescription rates might have occurred within counties during the study period, meaning that the number of relapses does not perfectly match county prescription rates by year. We therefore performed a sensitivity test where we calculated county lithium prevalences for the year 2015 only, and performed regression analyses for the combined population as well as for BD I group separately. These results are found in Additional file 1.
留言 (0)