
記住我
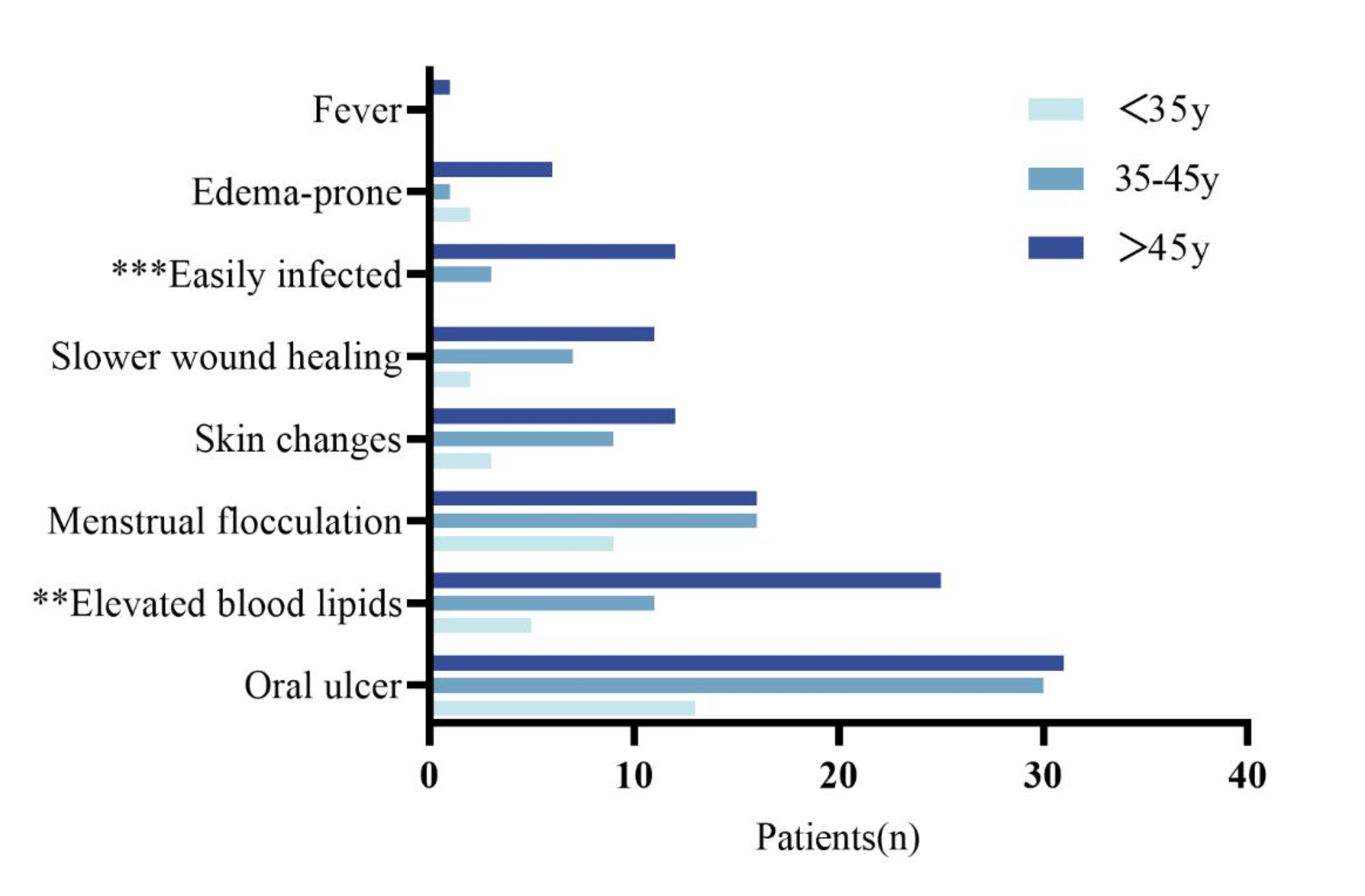




Characteristics of the 121 LAM patients are presented in Table 1. All patients were female, and 82.6% were over 35 years old. A total of 33.9% of LAM patients had an education level up to secondary school. Among the patients, 78.5% had children. Approximately 41.3% of patients had a monthly income of no more than 3000 RMB. Rapamycin was taken by 81.8% of patients, most of whom experienced adverse reactions such as oral ulcers, elevated blood lipids, and menstrual irregularities. Significant differences in adverse reactions, such as elevated blood lipids and susceptibility to infections, were observed among patients of different age groups (p ≤ 0.01) (Fig. 1). Additionally, 41.3% of patients required home oxygen therapy, and 46.3% underwent surgical procedures. Furthermore, 37.2% of patients had a disease duration of more than 7 years.
Table 1 Demographic and clinical data on the 121 LAM patientsFig. 1
Side effects in patients with LAM who took rapamycin at different ages(n = 99). **P ≤ 0.01, ***P ≤ 0.001
Severity and health care useA total of 80.2% of LAM patients reported experiencing dyspnea on most days (Table 1). Activity limitation was severe, with 65.3% patients reporting work limitation or inability to work because of LAM. Nearly all patients reported being hospitalized for LAM in the past year, and 26.5% described to have been hospitalized more than three times.
Present symptomsThe present symptoms most of the time in the past year in 121 LAM patients (99 patients take rapamycin, 22 patients do not take rapamycin) with different disease courses that divided into five courses are illustrated in Fig. 2. In patients taking rapamycin (Fig. 2A), symptoms mostly include shortness of breath, chest tightness, and cough, with hemoptysis being rare. Among patients with a disease duration exceeding 7 years, all symptoms except pneumothorax are most commonly observed, and there is a significant difference in the incidence of pneumothorax symptoms. And patients with a disease duration of more than 7 years are also the most common among those with no symptoms. In contrast, in patients not taking rapamycin (Fig. 2B), most do not exhibit any symptoms, or they experience shortness of breath and chest tightness, with no cases of hemoptysis. Additionally, patients with a disease duration of 1–3 years tend to have more discomfort symptoms.
Fig. 2
Present symptoms most of the time in the past year in 121 LAM patients with different disease durations: (A) taking rapamycin; (B) not taking rapamycin. ** p ≤ 0.01
Illness cognitionThe scores for the three dimensions of the ICQ were as follows: helplessness (15.74 ± 4.68) points; acceptance (16.00 ± 3.28) points; perceived benefits (16.92 ± 3.86) points. Single-factor analysis of variance (Table 2) revealed significant correlations between educational level, age grope, monthly household income, rapamycin use, home oxygen therapy, number of hospitalizations, disease duration, current degree of dyspnea, activity limitation from LAM and patients’ sense of helplessness in LAM (p ≤ 0.05). The number of children was significantly correlated with patients’ acceptance scores (p ≤ 0.05). Whether surgery had been performed was significantly correlated with patients’ acceptance and perceived benefits levels (p ≤ 0.05).
Table 2 Results of univariate analysis of the illness cognition questionnaire (ICQ) subscale scores and related factors in the 121 LAM patients (only statistically significant results are shown)Factors with p ≤ 0.05 in the single-factor analysis were included in the multiple regression analysis (Table 3), with “entry” used for sub-variables and “stepwise entry” for other variables. Multiple regression analysis found that patients’ disease duration and activity restriction entered the regression equation for the helplessness dimension, while whether surgery had not been performed entered the regression equation for the perceived benefits dimension (R2=0.02). However, no factors entered the regression equation for the acceptance dimension.
Table 3 Results of multivariate regression analysis of the illness cognition questionnaire subscale scores and related factors in the 121 LAM patients( n = 121)Furthermore, factors with p ≤ 0.05 in the multiple regression analysis were subjected to partial correlation analysis (Table 4), revealing a significant correlation between patients’ disease duration, activity restriction (p ≤ 0.00), and their sense of helplessness in LAM illness cognition.
Table 4 Relationship of activity limitation from LAM and disease duration with the illness cognition questionnaire scores of the 121 LAM patients on the items of " helplessness “, " acceptance " and " perceived benefits” ( n = 121)Illness perceptionThe average score of the BIPQ is 45.43 ± 8.97, with consequences score of 5.97 ± 2.78; timeline score of 8.76 ± 2.24; personal control score of 4.12 ± 2.54; treatment control score of 3.20 ± 2.21; identity score of 6.72 ± 2.33; concern score of 7.98 ± 2.23; understanding score of 2.94 ± 2.15; and emotional response score of 5.73 ± 2.59.
Single-factor analysis of variance (Table 5) revealed significant correlations between patients’ age, family monthly income, economic burden, use of rapamycin, use of home oxygen therapy, disease duration, severity of respiratory distress, activity limitation, and consequences scores (p ≤ 0.05). Significant correlations were also found between patients’ age, use of rapamycin, disease duration, and timeline scores (p ≤ 0.05). Furthermore, disease duration, presence of chylous effusion, and treatment control scores showed significant correlations (p ≤ 0.05). Significant correlations between patients’ age, presence of chylous effusion, use of rapamycin, use of home oxygen therapy, disease duration, history of surgical treatment, severity of respiratory distress, activity limitation, and identity scores were observed (p ≤ 0.05). Moreover, the use of home oxygen therapy showed significant correlations with concern scores (p ≤ 0.05). Additionally, the presence of pneumothorax, use of home oxygen therapy, disease duration, and understanding scores showed significant correlations (p ≤ 0.05). Lastly, disease duration, presence of renal angiomyolipoma, use of rapamycin, use of home oxygen therapy, severity of respiratory distress, activity limitation, and emotional response scores were significantly correlated (p ≤ 0.05). No features were found to be related to personal control scores in the survey.
Table 5 Results of univariate analysis of the brief illness perception Questionnaire(BIPQ) subscale scores and related factors in the 121 LAM patients (only statistically significant results are shown)In single-factor analysis, factors with p ≤ 0.05 entered multiple regression analysis (Table 6), with “enter” used as a subvariable and other variables as “stepwise entry.” Multiple regression analysis found that patient disease duration, whether taking rapamycin, whether home oxygen therapy and activity limitation entered the “consequences” regression equation (p ≤ 0.01); disease duration entered the “timeline” regression equation(P ≤ 0.00); whether having had chylous effusion and disease duration entered the “treatment control” regression equation (p ≤ 0.01; age, whether taking rapamycin, and activity limitation entered the “identity” regression equation (p ≤ 0.05); whether home oxygen therapy entered the “concern” regression equation (p ≤ 0.05); whether having had pneumothorax entered the “understanding” regression equation (p ≤ 0.05); whether taking rapamycin, whether home oxygen therapy and activity limitation entered the “emotional response” regression equation (p ≤ 0.05); however, no factors entered the “personal control” regression equation.
Table 6 Results of multivariate regression analysis of the brief illness perception Questionnaire subscale scores and related factors in the 121 LAM patients( n = 121)Further, factors with p ≤ 0.05 from multiple regression analysis were entered into partial correlation analysis (Table 7), revealing that identity and emotional response scores were significantly correlated with whether taking rapamycin (p ≤ 0.05); consequences, identity, concern, understanding, and emotional response scores were significantly correlated with home oxygen therapy (p ≤ 0.05); consequences and treatment control scores were significantly correlated with disease duration (p ≤ 0.05); furthermore, consequences and identity scores were significantly correlated with activity limitation (p ≤ 0.05).
Table 7 Relationship of taking rapamycin, home oxygen therapy, disease duration and activity limitation with the brief illness perception questionnaire scores of the 121 LAM patients on the items of “consequences”, “timeline”, “treatment control”, “identity”, “concern”, “understanding” and “emotional response” (n = 121)
留言 (0)