
記住我
Healthcare worker (HCW) well-being is of great public health importance as high rates of burnout are present throughout the medical field and are linked to poor patient care outcomes (1). Burnout can be defined as unsuccessfully managed chronic workplace stress that results in emotional exhaustion, job dissatisfaction, and reduced professional efficacy (2). Systemic factors such as workload, organizational structure, and access to support systems contribute to stress and burnout rates. Since the COVID-19 pandemic, well-being has taken center stage due to concerning levels of psychosocial strain throughout the healthcare workforce. A study by the United States Centers for Disease Control and Prevention (CDC) reported significantly higher burnout rates among health workers in 2022 (46%) compared to 2018 (32%) (3). In the global context, a report by the Qatar Foundation, World Innovation Summit for Health (WISH), in collaboration with the World Health Organization (WHO) found similar findings of healthcare worker burnout ranging from 41 to 52% (4). Other measures such as the number of poor mental health days, intent to change jobs, and harassment showed similar trends before and after the pandemic (3).
The negative impact on quality and costs of care associated with poor HCW well-being is also of significant concern (1). HCWs suffering from burnout may struggle to concentrate and be less detail-oriented, and more likely to make mistakes that can affect patient care and increase medical expenditures (5). Multiple studies have demonstrated a relationship between the onset of physician burnout and declining patient safety (6, 7). A systematic review by Hall et al. found that “poor [well-being] and moderate to high levels of burnout [were] associated, in the majority of studies reviewed, with poor patient safety outcomes.” (6) Increases in the frequency of hospital-acquired infections (8), mortality risk, and length of hospital stay have all been found to be associated with nurse burnout (9). A cost–benefit analysis of an institution-wide support program for nursing staff projected an estimated $1.81 million in annual hospital cost savings after implementation of the well-being intervention (10). Given these concerning findings, it is imperative to address well-being among HCWs.
Minority healthcare workers (MHCW), such as those self-identifying with racial/ethnic, sexual and gender, or migrant minority groups, face unique challenges that may affect their workplace associated well-being. In addition to traditional workplace pressures, MHCW may need to navigate systemic barriers such as structural racism, discrimination, and stereotyping. Further, they are more likely to work in underserved communities with limited resources (11). These circumstances may compound one another and contribute to differences in well-being compared to their non-minority counterparts. Although it is crucial to acknowledge the unique circumstances of this population, there is inconclusive evidence that MHCW experience worse well-being. Previous studies present conflicting evidence on burnout rates between minority and non-minority HCWs with some even suggesting that a minority background can be a protective factor (12).
There is limited data on interventions targeting the well-being of MHCW. Most well-being interventions are designed as one-size-fits-all solutions intended to apply to all workers. It may be important to implement targeted interventions that address the distinct needs of MHCW. By doing so, all HCWs, regardless of their sociodemographic backgrounds or identities, could feel supported and continue to provide high-quality care for their patients. The aim of this study was to identify and examine interventions specifically designed to support the well-being of MHCW. Additionally, the study analyzed existing literature on well-being outcomes and experiences comparing minority and non-minority HCWs.
MethodsThis systematic review was conducted between November 2023 and April 2024 in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, 2021) (13) guidelines. The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO, ID# CRD42023478339) prior to commencement of data collection.
Search strategyA comprehensive literature search was performed using the following databases: PubMed, Medline, Scopus, Embase, PsycINFO, Web of Science, CINAHL, ProQuest Dissertations and Theses Global, American Doctoral Dissertations, and Open Access Theses and Dissertations. Additional sources such as databases of gray literature, volumes of journals, reference lists of books, book chapters, systematic reviews were also searched. No time or study design restrictions were applied. The search was limited to availability in English. Multiple key terms and Boolean operators such as minority, underrepresented, healthcare worker, well-being, mental health, intervention, and program were used to target relevant papers. Results were limited to publications that included the search terms within their title or abstract text. The reference lists of eligible articles were also hand-searched to identify any additional publications. The detailed search strategy by database is included in Supplementary 1.
Eligibility criteriaPublished papers reporting original or secondary results of quantitative, qualitative, or mixed-methods research on the well-being of MHCW and targeted program interventions for MHCW were included. All study designs were considered inclusive of other systematic or scoping reviews in an effort to synthesize high-level evidence and reduce duplication of effort. We defined HCWs to be inclusive of physicians, pharmacists, physician assistants, nurses, hospital faculty, and their corresponding students or trainees. We chose to include early-career groups such as students as literature suggests early onset of burnout (14). Similarly, a broad characterization of minority was utilized to include racial/ethnic, gender, sexual, and migrant minority groups. These were defined within the geographic and cultural contexts in which the studies were conducted. The wide-ranging definitions were used capture more relevant data since published literature on this topic are relatively scarce. For inclusion in this review, articles must have included MHCW well-being outcomes or an intervention targeting the well-being of MHCW. Table 1 provides the detailed inclusion and exclusion criteria utilized to determine study eligibility.
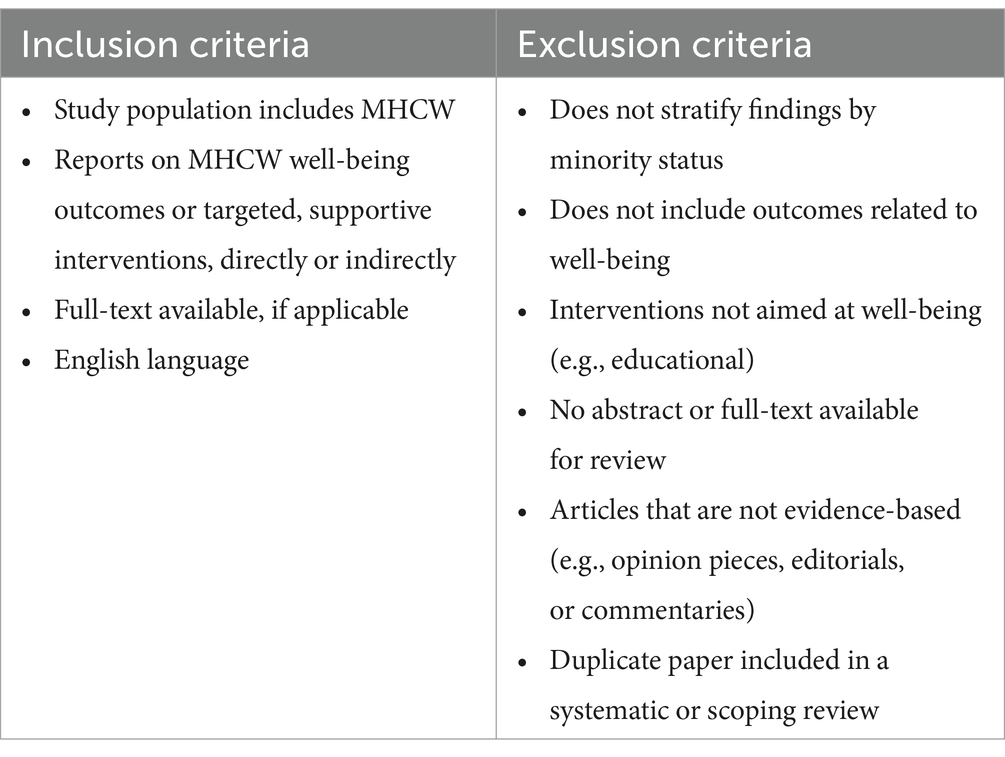
Table 1. Inclusion and exclusion criteria.
Study selection and data extractionAn online systematic review management system, Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia), was utilized for literature screening and data extraction. There were four reviewers, MM, TB, MC, and WH. Two independent reviewers conducted each title/abstract screening and full-text review. In cases of disagreement, consensus was acquired through discussion. At least one reviewer completed data extraction for selected articles. Extracted data included study title, author(s), date of publication, country, study design, type of HCW, type of MHCW, number of participants, attrition and response rate, well-being measures or interventions, well-being related primary and secondary outcomes (if applicable), and lessons learned.
Data synthesisExtracted information was exported from Covidence to Microsoft Excel (version 16.81). A spreadsheet was used for organization of the extracted data with a focus on relevant variables. Meta-analysis was not possible due to heterogeneity in the methodological features of the studies. Therefore, descriptive analysis of the included papers was conducted.
Quality assessmentIncluded studies were categorized as quantitative (randomized, non-randomized, or descriptive), qualitative, mixed-methods, or systematic/scoping review. Due to the variety of study designs included in this review, two comprehensive critical appraisal tools, the Mixed Methods Appraisal Tool (MMAT, version 2018) (15, 16) and the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Systematic Reviews and Research Syntheses (2015) (17), were utilized. Two reviewers independently assessed all studies and disagreements were addressed through discussion to achieve consensus.
The MMAT is designed for the assessment of five study types: qualitative, quantitative randomized control, quantitative non-randomized, quantitative descriptive, and mixed-methods studies. There are two screening questions: (1) “Are there clear research questions?” and (2) “Do the collected data allow to address the research questions?” (15). The screening questions are followed by 25 appraisal items addressing quality criteria split into five sections corresponding to the specific study design, with each section having five questions. A total of five appraisal items are answered for all qualitative and quantitative study designs. A total of 15 questions are assigned for mixed-method studies as the specific two study designs included plus the mixed-methods-specific questions must be answered; however, the lowest score of the three categories is considered the overall quality. Response options to the series of questions include ‘yes’, ‘no’, or ‘cannot tell’. The full set of assessment questions can be found elsewhere (15). Quality was categorized as low (MMAT score, 0–2), moderate (MMAT score, 3–4), or high (MMAT score, 5).
The JBI tool was utilized for the quality appraisal of systematic reviews and scoping reviews. This tool has a total of 11 items with response options of ‘yes’, ‘no’, ‘unclear’, or ‘not applicable’. Overall quality was reported based on percentage of criteria as low (<40%), moderate (40–80%), or high (>80%).
Results Study selectionThe initial search produced 3,815 records, of which 1,837 duplicates were removed (Figure 1). After screening of the available abstracts and titles by two independent reviewers, 147 studies were eligible for full-text review. Of these, 104 were excluded for various reasons (detailed in Figure 1) resulting in 43 included studies.
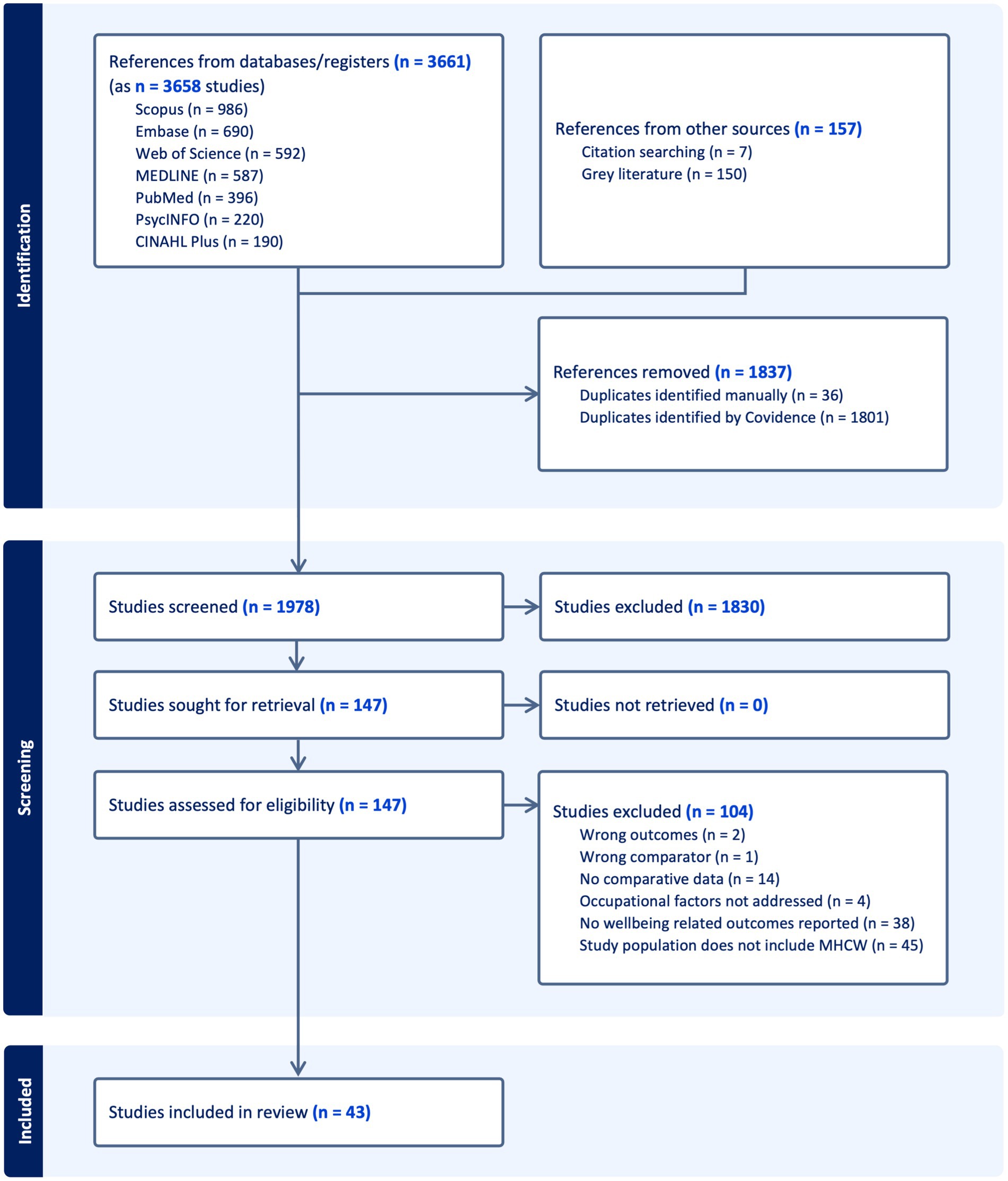
Figure 1. PRISMA diagram illustrating the search for relevant studies at different stages including identification, selection, and inclusion of the studies based on predefined criteria.
Study characteristicsAll 43 included studies were written in English and published between 2006 and 2023. Most of the studies (67.4%) utilized quantitative descriptive methods, 7 (16.3%) qualitative, 3 (7.0%) systematic or scoping reviews, 2 (4.7%) quantitative non-randomized, and 2 (4.7%) were mixed-methods studies. No studies utilized a randomized design. Geographic location was mostly the United States (81.4%) followed by Canada (7.0%) and the United Kingdom (4.7%). Other countries included Germany, Israel, and Malaysia. There was wide variability in the types of healthcare professionals included: physicians, medical trainees (fellows, residents, and students), nurses, health department employees, physician scientists, and other clinical-based students. A majority of studies defined minority status by race/ethnicity. Table 2 summarizes the key characteristics of the included studies.
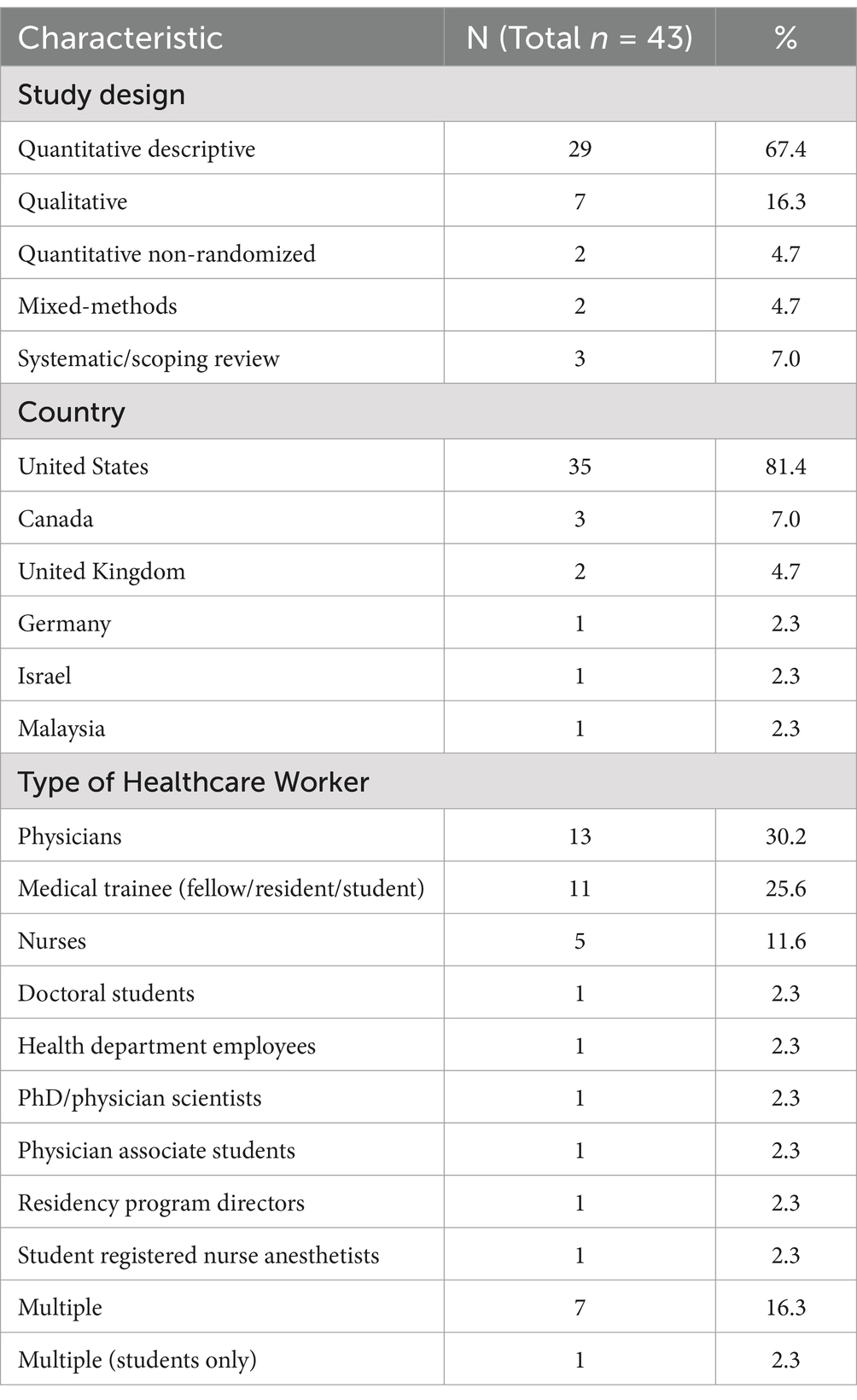
Table 2. Characteristics of included studies.
Studies measured several well-being domains such as burnout, emotional exhaustion, depersonalization, job satisfaction, intent to leave, depression, anxiety, and discrimination. Many authors created their own questionnaires or adapted already existing ones. Burnout was the most commonly assessed well-being outcome. Multiple validated and non-validated tools were utilized in assessing burnout; 10 studies utilized the Maslach Burnout Inventory (MBI) (18) and 5 used the Copenhagen Burnout Inventory (CBI) (19). All authors used paper-and-pencil or web-based/electronic self-report questionnaires and nine studies used semi-structured interviews to identify qualitative themes. A majority of studies used convenience sampling to identify participants, however we included data from 4 large national systematic surveys that compare well-being measures for racial/ethnic minority and non-minority HCWs.
Study qualityThe MMAT was used to evaluate 40 studies (Table 3). All of these had a response of ‘yes’ to the two screening questions, which were not included in Table 3. MMAT questions 2.1 to 2.5 were also not included as no studies met the design criteria. All primary studies met more than half of the quality criteria of MMAT and used an appropriate sample frame to address the target population. However, the adequacy of the sample size and the use of valid methods was unclear for several studies. Two systematic reviews and 1 scoping review used the JBI appraisal tool. Table 4 shows appraisal results of JBI-evaluated studies. Overall, 76.7% of the included studies were of moderate methodological quality and 23.3% were of high quality. No studies were rated as low quality.
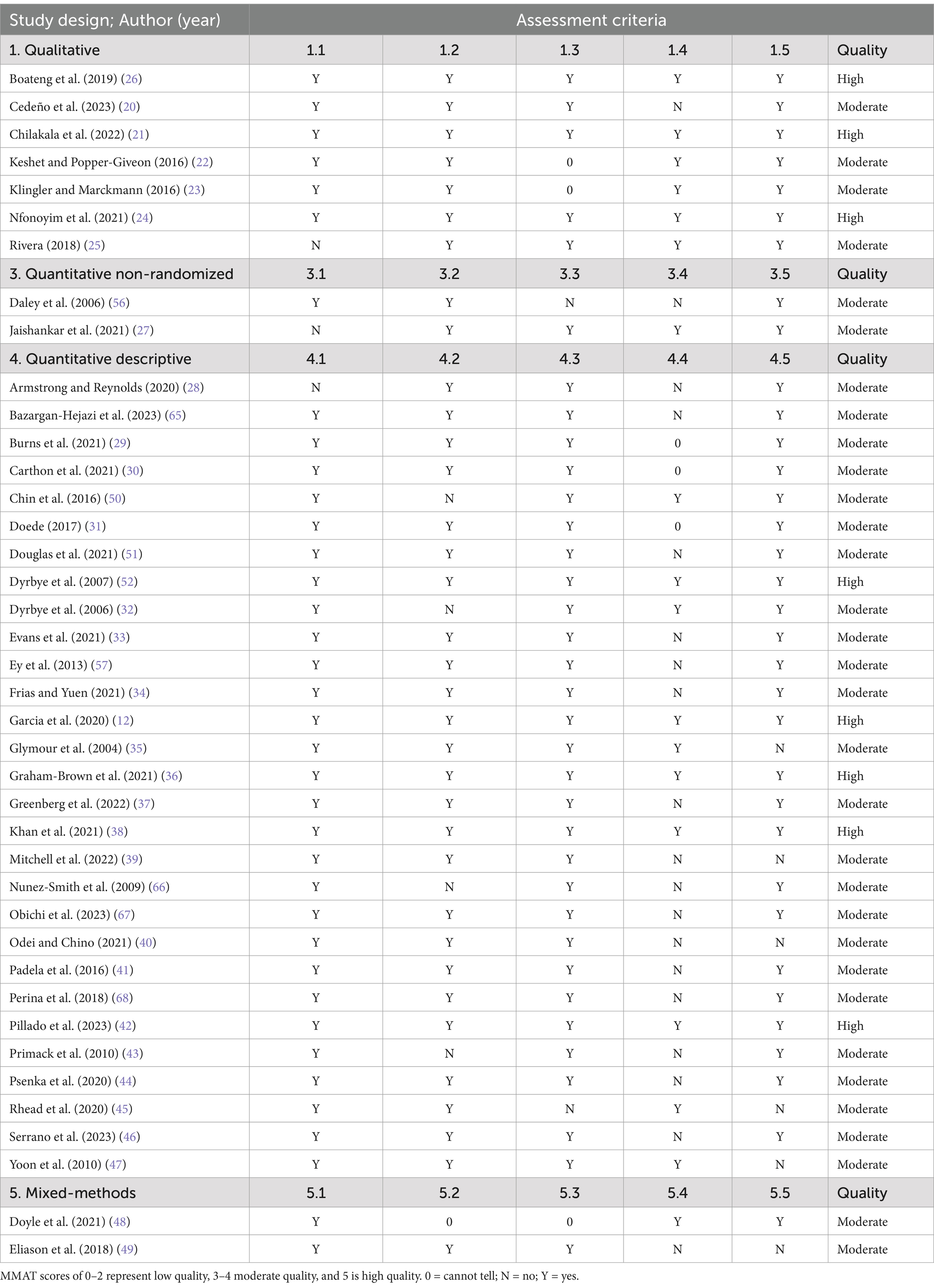
Table 3. Appraisal of quantitative, qualitative, and mixed-method studies using MMAT.
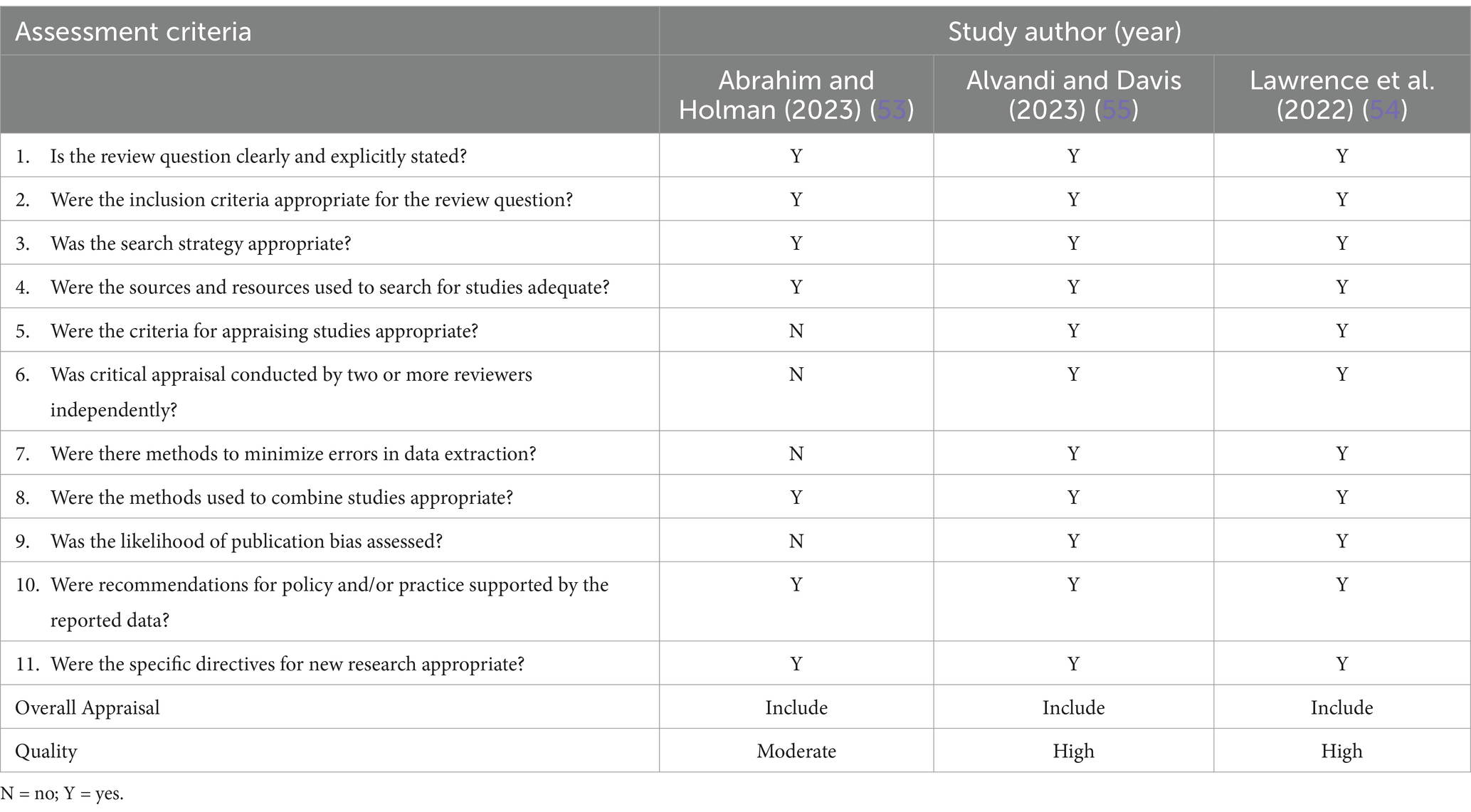
Table 4. Appraisal of systematic and scoping reviews using JBI critical appraisal checklist for systematic reviews and research syntheses.
Study outcomes Well-being in minority versus non-minority HCWsMost qualitative studies (85.7%) did not have non-minority comparison groups, however all identified negative experiences for MHCW (20–25). The qualitative themes identified included exposure to microaggressions, institutional ostracizing, tense working environment, racial isolation, lack of culturally diverse mentors, stereotypical or offensive attitude from patients, unprofessional encounters from peers, pressure to prove themselves as a result of negative experiences, and fear of being othered. Experiences of microaggression and discrimination were reported by both racial/ethnic and gender/sexual MHCW.
A majority of studies (n = 29, 67.4%) compared the well-being of minority and non-minority HCWs either qualitatively or quantitively. Of these, the vast majority (82.8%) noted some worse outcomes in the MHCW population (26–49). One study found no significant overall difference in burnout by gender or ethnicity (50). Three studies reported better well-being among MHCW in comparison to their non-minority counterparts (12, 51, 52). Garcia et al. (12) reported lower adjusted odds of burnout among minority racial/ethnic groups in comparison to non-Hispanic white participants (Hispanic/Latinx physicians, odds ratio [OR] = 0.63, 95% confidence interval [CI] [0.47, 0.86]; non-Hispanic Black physicians, OR = 0.49, 95% CI [0.30, 0.79]). This study was a secondary analysis of survey data from 4,424 physicians, using MBI to assess burnout. Authors noted several limitations including a much lower response rate for minority physicians and the utilization of the American Medical Association’s Physician Masterfile dataset to identify minority physicians, which lacked comprehensive racial/ethnic information. Additionally, Abrahim and Holman (53) conducted a scoping review of literature on the well-being of racial and ethnic minority nurses during the COVID-19 pandemic. Two studies in their review documented greater anxiety among white nurses, but contained relatively small, predominantly white, unrepresentative samples. The authors concluded that “findings for the nurses of color may not be reliable because the samples included few racial and ethnic minority nurses.” (53).
In regards to overall burnout scores, two studies found no significant difference between minority and non-minority medical students (28, 32). However, one of these studies (28) (n = 162) showed significantly higher rates of personal burnout among racial/ethnic minority medical students (p = 0.001). The second study (32) surveyed medical students (n = 545) and although there were similarly no overall differences in burnout, emotional exhaustion, or depersonalization, minority medical students had a significantly lower sense of personal accomplishment (42% vs. 28%; p = 0.02). Also of note, minority students were less likely to respond to the survey (37% vs. 50%; p < 0.001).
A systematic review by Lawrence et al. (54) that focused on the racial/ethnic differences in burnout rates had inconclusive findings, and recommended increased evaluation and focus on systemic factors that may be at play. Three of the 16 studies in this review did not include HCWs. Additionally, Lawrence et al. noted that their findings were nuanced and several of the included studies had methodological issues.
The majority of studies used convenience sampling to identify participants, but our sample also included data from four large national systematic surveys that compared well-being measures for racial minority and non-minority HCWs. The largest of these (31) (n = 27,953) was from the National Sample Survey of Registered Nurses. It found that Asians had lower odds (p < 0.001) of job dissatisfaction and having changed jobs (p < 0.001) compared to white counterparts, while Black and Hispanic participants showed no significant association. The authors concluded that race/ethnicity was a predictor of job satisfaction and turnover and Asian nurses showed more positive outcomes than white nurses, while Black and Hispanic individuals showed significantly worse outcomes. Another large national survey (30) (n = 14,778) reporting on the data from RN4CAST-U.S found that Black nurses reported greater job dissatisfaction (p < 0.001) and intent to leave within a year (p < 0.001) in comparison to white nurses. A national training survey from the UK General Medical Council of 627 renal medicine physicians similarly suggested that racial/ethnic minority medical trainees reported higher burnout rates than white trainees (36).
However, data from a national physician survey (n = 3,096) from the American Board of Family Medicine (ABFM) Family Medicine Continuing Certification Examination Registration questionnaire showed that minority physicians were significantly less likely to report depersonalization, both as a binary variable (p = 0.03) and continuous variable (p < 0.001), less likely to report emotional exhaustion as a continuous variable (p = 0.04), but equally likely to report emotional exhaustion (p = 0.09) (51). Minority physicians were more likely to work in counties with higher diversity index and authors concluded that working in racially and ethnically diverse environments could be a mediating factor resulting in a lower frequency of emotional exhaustion and feelings of depersonalization (51).
Among studies that compared outcomes between men and women (n = 16), 68.8% found worse well-being among women HCWs. Yoon et al. (47) explored conflict as a correlate of burnout among HCWs. No association was found between conflict over treatment decisions and race/ethnicity, but there was a significant positive association among women physicians. Reasons for this association are not well understood, but Yoon et al. (47) suggest that female patients are more likely to choose female physicians and more willing to voice disagreements with physicians of the same gender. Five studies specifically investigated gender differences in burnout. Two of these studies did not find any difference in burnout among male and female HCWs (38, 50). One study found that male renal trainees reported higher burnout rates than women colleagues (36). However, a systematic review of 11 studies by Alvandi and Davis (55) showed that female HCWs reported greater burnout.
Sexual minority HCWs were examined in four studies. Key findings include discomfort in ‘coming-out’ in the workplace (49), being socially excluded (25), and greater odds of depressive or anxiety symptoms than heterosexual counterparts (33).
Well-being interventionsOnly one study, by Daley et al. (56) included a specific MHCW-focused well-being intervention. They examined the change in retention rate among health center faculty after the implementation of the Junior Faculty Development Program for minority-identifying faculty which provided development workshops, counseling, and mentoring. There was a non-significant increase in retention rate of 15% among minority-identifying faculty in academic medicine. One other study by Ey et al. (57) included an intervention that was not tailored to the MHCW population. They evaluated a Resident Wellness Program that provided free, on-site counseling for all medical trainees regardless of minority status. Findings indicated that MHCW were significantly less likely to utilize the program.
Details of study population, measures, outcomes, and lessons learned of all included studies are summarized in Supplementary 2.
DiscussionContrary to our expectations, there were few publications on supportive interventions that specifically target MHCW. We found only one published MHCW-specific intervention, a development and mentorship program which showed no significant association with retention rate (56). Instead, findings from this review suggest that creating a safe work environment and empowering MHCW to participate in well-being interventions may be important. One study (57) showed that MHCW were less likely that their non-minority counterparts to utilize their well-being program. Several studies found discomfort among HCWs in receiving support, and that time away from work may be a potential barrier to utilizing well-being programs (57, 58). These barriers may be greater for MHCW experiencing discrimination and other systemic challenges, who may want to avoid any additional discomfort in the workplace.
To our knowledge, this is the first systematic review to comprehensively explore the well-being of MHCW. We aimed to cover a broad topic area as we felt that any narrowing of the well-being definition may result in selection bias. The search included a broad range of search terms with minimal limitations. All study designs were included and no studies were excluded based on quality. Uniformity in the critical appraisal process was prioritized by usage of the MMAT which encompassed most study designs. This important review provided context and awareness to how intersectional factors (e.g., race, gender, sexual orientation) affects the well-being of the minority-identifying healthcare workforce, highlighting the importance of inclusivity and equity in the workplace and providing evidence-based syntheses for policymakers to improve the well-being of MHCW.
Consistent with previous literature, we found inconsistencies in well-being outcomes among MHCW. There are potential reasons for these discrepant findings. It is important to consider that minority populations may express stress differently which could affect scores on well-being measures. The validity of previously established stress models has been questioned for minority populations. Ivey and Gauch (59) demonstrated that “minority communities have different distributions of emotions than the general population” and that existing models may not be representative as they are not trained with minority-specific data. Singh et al. (60) found that chronic stress among individuals who experience continuous discrimination leads to emotional dysregulation and emotional suppression. They argued that the “impact of any instance of social isolation, discrimination, and bias is directly responsible for suppression of emotional expression” (60) whether that be negative or positive responses. This potential reporting bias should be considered in interpreting our findings.
Notably, larger, well-represented national surveys tended to find higher rates of burnout among MHCW. It also appeared that burnout among MHCW can be modulated by a variety of professional and environmental factors. For example, working in racially and ethnically diverse environments was found to be a mediating factor reducing burnout among minority family physicians (51). MHCW may feel less minoritized in settings that promote diversity. Similarly, in a survey of 519 oncologists, 48 minority radiation oncologists reported greater burnout rates than non-minority, but minority medical oncologists reported lower burnout rates than non-minority respondents. This suggests a potential influence of differences in work environment on burnout (40).
Psychological distress can be cumulative over the life course and can also be compounded by the presence of multiple stressors. For example, identifying with more than one type of minority or identifying with an ‘invisible’ minority group may be associated with worse outcomes. Those identifying as sexual minorities, in particular, are sometimes able to make a ‘choice’ about coming-out to colleagues and patients, as opposed to those with racial/ethnic minority status which may be more visibly apparent. This could worsen well-being among the LGBTQ+ community as they internalize negative feelings. Future studies should control for or evaluate the differences associated with a particular minority group, however this is understandably challenging given the concept of intersectionality in identity. There is a complex interplay of various facets of identity, such as ethnicity, gender, sexuality, professional seniority, etc., that do not exist in isolation but rather intersect in various ways to shape an individual’s context (61).
There are multiple benefits to an inclusive and supportive work environment in promoting well-being among MHCW. Wolfe (62) theorizes that LGBTQ+ healthcare professionals, similar to other minority-identifying populations, encounter incongruence between their personal and professional identities, and thus have differential experiences with mental distress and burnout. They also call for “intersectional actions that recognize and mitigate spaces of inequality that constrain the benefit marginalized professionals receive from improvement efforts” (62) such as interventions tailored to specific minority group needs. Brown et al. (63) emphasize that medical education diversity goals are only attainable “when inclusion and equity are on the table as well” since a supportive work environment must address systemic inequalities in order to promote well-being among the workforce. Prioritizing diversity and inclusion policies requires a systemic approach of stakeholder collaboration, strategy evaluation, and community engagement (64). This will also have a direct impact on the retention of MHCW. Additionally, a healthcare workplace that closely represents the community it serves will improve the quality of care (64).
LimitationsThis study has some limitations. There was methodological heterogeneity in the types of well-being outcomes and the measurement tools included in studies. However, there was less heterogeneity in the study populations. Studies also utilized different definitions of “minority” with most focusing on racial/ethnic minorities, while others included immigration status and religious affiliation. This prevented aggregation or quantitative comparisons of results. Furthermore, findings from different countries were included in this review without consideration of the cultural, political, and economic contexts surrounding healthcare. Therefore, the results should be interpreted in context.
ConclusionThere is paucity of published evidence on supportive interventions to address MHCW well-being. The results of our review do not fully support the need for well-being programs tailored solely to MHCW. However, we could only find one study specifically supporting MHCW’s. It is possible that systematic barriers such as discrimination are preventing MHCW’s participation in support programs. Given the complex and intersectional nature of identity, it is understandable that there is no one “size” approach even among a particular population of MHCW. Rather, a broad public health approach should be considered to mitigate the negative health outcomes and improve utilization of support programs, including the development and implementation of policies surrounding diversity and inclusion, mental health services, and cultural competency. By increasing focus on the barriers to well-being faced by MHCW, the well-being of the entire healthcare workforce could be improved and subsequently translate into better patient care. We recommend future research on MHCW utilizing validated well-being measures and incorporating a wider geographical variation beyond North America and Europe, especially from underrepresented countries.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributionsTB: Formal analysis, Writing – original draft, Investigation, Methodology. MM: Formal analysis, Writing – original draft, Conceptualization, Writing – review & editing. MC: Formal analysis, Investigation, Writing – review & editing. WH: Data curation, Software, Writing – review & editing. CW: Methodology, Writing – review & editing. KW: Investigation, Methodology, Writing – review & editing. CC: Writing – review & editing. MB: Writing – review & editing. GE: Writing – review & editing. HM: Funding acquisition, Writing – review & editing. AW: Funding acquisition, Writing – review & editing.
FundingThe author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) [Thriving Together: Supporting Resilience in the Healthcare Workforce. 1U3MHP45382–01-00].
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statementThe authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1531090/full#supplementary-material
Footnotes References5. Patel, RS, Bachu, R, Adikey, A, Malik, M, and Shah, M. Factors related to physician burnout and its consequences: a review. Behav Sci (Basel). (2018) 8:98. doi: 10.3390/bs8110098
PubMed Abstract | Crossref Full Text | Google Scholar
6. Hall, LH, Johnson, J, Watt, I, Tsipa, A, and O’Connor, DB. Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. (2016) 11:e0159015. doi: 10.1371/journal.pone.0159015
PubMed Abstract | Crossref Full Text | Google Scholar
8. Cimiotti, JP, Aiken, LH, Sloane, DM, and Wu, ES. Nurse staffing, burnout, and health care-associated infection. Am J Infect Control. (2012) 40:486–90. doi: 10.1016/j.ajic.2012.02.029
PubMed Abstract | Crossref Full Text | Google Scholar
9. Schlak, AE, Aiken, LH, Chittams, J, Poghosyan, L, and McHugh, M. Leveraging the work environment to minimize the negative impact of nurse burnout on patient outcomes. Int J Environ Res Public Health. (2021) 18:610. doi: 10.3390/ijerph18020610
PubMed Abstract | Crossref Full Text | Google Scholar
10. Moran, D, Wu, AW, Connors, C, Chappidi, MR, Sreedhara, SK, Selter, JH, et al. Cost-benefit analysis of a support program for nursing staff. J Patient Saf. (2020) 16:e250–4. doi: 10.1097/PTS.0000000000000376
PubMed Abstract | Crossref Full Text | Google Scholar
11. Xierali, IM, and Nivet, MA. The racial and ethnic composition and distribution of primary care physicians. J Health Care Poor Underserved. (2018) 29:556–70. doi: 10.1353/hpu.2018.0036
PubMed Abstract | Crossref Full Text | Google Scholar
12. Garcia, LC, Shanafelt, TD, West, CP, Sinsky, CA, Trockel, MT, Nedelec, L, et al. Burnout, depression, career satisfaction, and work-life integration by physician race/ethnicity. JAMA Netw Open. (2020) 3:e2012762. doi: 10.1001/jamanetworkopen.2020.12762
PubMed Abstract | Crossref Full Text | Google Scholar
16. Hong, QN, Pluye, P, Fàbregues, S, Bartlett, G, Boardman, F, Cargo, M, et al. Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study. J Clin Epidemiol. (2019) 111:49–59.e1. doi: 10.1016/j.jclinepi.2019.03.008
PubMed Abstract | Crossref Full Text | Google Scholar
17. Aromataris, E, Fernandez, R, Godfrey, CM, Holly, C, Khalil, H, and Tungpunkom, P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. JBI Evidence Implementation. (2015) 13:132–40. doi: 10.1097/XEB.0000000000000055
PubMed Abstract | Crossref Full Text | Google Scholar
19. Kristensen, TS, Borritz, M, Villadsen, E, and Christensen, KB. The Copenhagen burnout inventory: a new tool for the assessment of burnout. Work Stress. (2005) 19:192–207. doi: 10.1080/02678370500297720
Crossref Full Text | Google Scholar
20. Cedeño, B, Shimkin, G, Lawson, A, Cheng, B, Patterson, DG, and Keys, T. Positive yet problematic: lived experiences of racial and ethnic minority medical students during rural and urban underserved clinical rotations. J Rural Health. (2023) 39:545–50. doi: 10.1111/jrh.12745
Crossref Full Text | Google Scholar
21. Chilakala, A, Camacho-Rivera, M, and Frye, V. Experiences of race-and gender-based discrimination among black female physicians. J Natl Med Assoc. (2022) 114:104–13. doi: 10.1016/j.jnma.2021.12.008
PubMed Abstract | Crossref Full Text | Google Scholar
23. Klingler, C, and Marckmann, G. Difficulties experienced by migrant physicians working in German hospitals: a qualitative interview study. Hum Resour Health. (2016) 14:57–7. doi: 10.1186/s12960-016-0153-4
PubMed Abstract | Crossref Full Text | Google Scholar
24. Nfonoyim, B, Martin, A, Ellison, A, Wright, JL, and Johnson, TJ. Experiences of underrepresented faculty in pediatric emergency medicine. Acad Emerg Med. (2021) 28:982–92. doi: 10.1111/acem.14191
PubMed Abstract | Crossref Full Text | Google Scholar
26. Boateng, G, Schuster, R, and Boateng, M. Uncovering a health and wellbeing gap among professional nurses: situated experiences of direct care nurses in two Canadian cities. Soc Sci Med. (2019) 242:112568. doi: 10.1016/j.socscimed.2019.112568
PubMed Abstract | Crossref Full Text | Google Scholar
27. Jaishankar, D, Dave, S, and Tatineni, S. Burnout, stress, and loneliness among u.s. medical students during the COVID-19 pandemic: a national survey. J Gen Intern Med. (2021) 36:1–469. doi: 10.1007/s11606-021-06830-5
PubMed Abstract | Crossref Full Text | Google Scholar
29. Burns, KEA, Pattani, R, Lorens, E, Straus, SE, and Hawker, GA. The impact of organizational culture on professional fulfillment and burnout in an academic department of medicine. PLoS One. (2021) 16:e0252778. doi: 10.1371/journal.pone.0252778
PubMed Abstract | Crossref Full Text | Google Scholar
30. Carthon, JMB, Travers, JL, Hounshell, D, Udoeyo, I, and Chittams, J. Disparities in nurse job dissatisfaction and intent to leave: implications for retaining a diverse workforce. J Nurs Adm. (2021) 51:310–7. doi: 10.1097/NNA.0000000000001019
PubMed Abstract | Crossref Full Text | Google Scholar
31. Doede, M. Race as a predictor of job satisfaction and turnover in US nurses. J Nurs Manag. (2017) 25:207–14. doi: 10.1111/jonm.12460
Crossref Full Text | Google Scholar
32. Dyrbye, LN, Thomas, MR, Huschka, MM, Lawson, KL, Novotny, PJ, Sloan, JA, et al. A multicenter study of burnout, depression, and quality of life in minority and nonminority US medical students. Mayo Clin Proc. (2006) 81:1435–42. doi: 10.4065/81.11.1435
PubMed Abstract | Crossref Full Text | Google Scholar
33. Evans, KE, Holmes, MR, Prince, DM, and Groza, V. Social work doctoral student well-being during the COVID-19 pandemic: a descriptive study. Int J Dr Stud. (2021) 16:569–92. doi: 10.28945/4840
Crossref Full Text | Google Scholar
34. Frias, D, and Yuen, CX. The physician assistant student experience: diversity, stress, and school membership. J Physician Assist Educ. (2021) 32:113–5. doi: 10.1097/JPA.0000000000000362
PubMed Abstract | Crossref Full Text | Google Scholar
35. Glymour, MM, Saha, S, and Bigby, J. Physician race and ethnicity, professional satisfaction, and work-related stress: results from the physician Worklife study. J Natl Med Assoc. (2004) 96:1283–94.
PubMed Abstract | Google Scholar
36. Graham-Brown, MP, Beckwith, HK, O’Hare, S, Trewartha, D, Burns, A, and Carr, S. Impact of changing medical workforce demographics in renal medicine over 7 years: analysis of GMC national trainee survey data. Clin Med (Lond). (2021) 21:e363–70. doi: 10.7861/clinmed.2020-1065
PubMed Abstract | Crossref Full Text | Google Scholar
37. Greenberg, AL, Cevallos, JR, Ojute, FM, Davis, DL, Greene, WR, and Lebares, CC. The general surgery residency experience: a multicenter study of differences in wellbeing by race/ethnicity. Ann Surg Open. (2022) 3:e187. doi: 10.1097/AS9.0000000000000187
PubMed Abstract | Crossref Full Text | Google Scholar
38. Khan, N, Palepu, A, Dodek, P, Salmon, A, Leitch, H, Ruzycki, S, et al. Cross-sectional survey on physician burnout during the COVID-19 pandemic in Vancouver, Canada: the role of gender, ethnicity and sexual orientation. BMJ Open. (2021) 11:e050380. doi: 10.1136/bmjopen-2021-050380
留言 (0)