
記住我

We conducted a bicentric prospective, feasibility and safety study to evaluate bilateral ACC-DBS combined with unilateral sensory thalamic-DBS in patients suffering from refractory unilateral NP. Study protocol has been previously published [19].
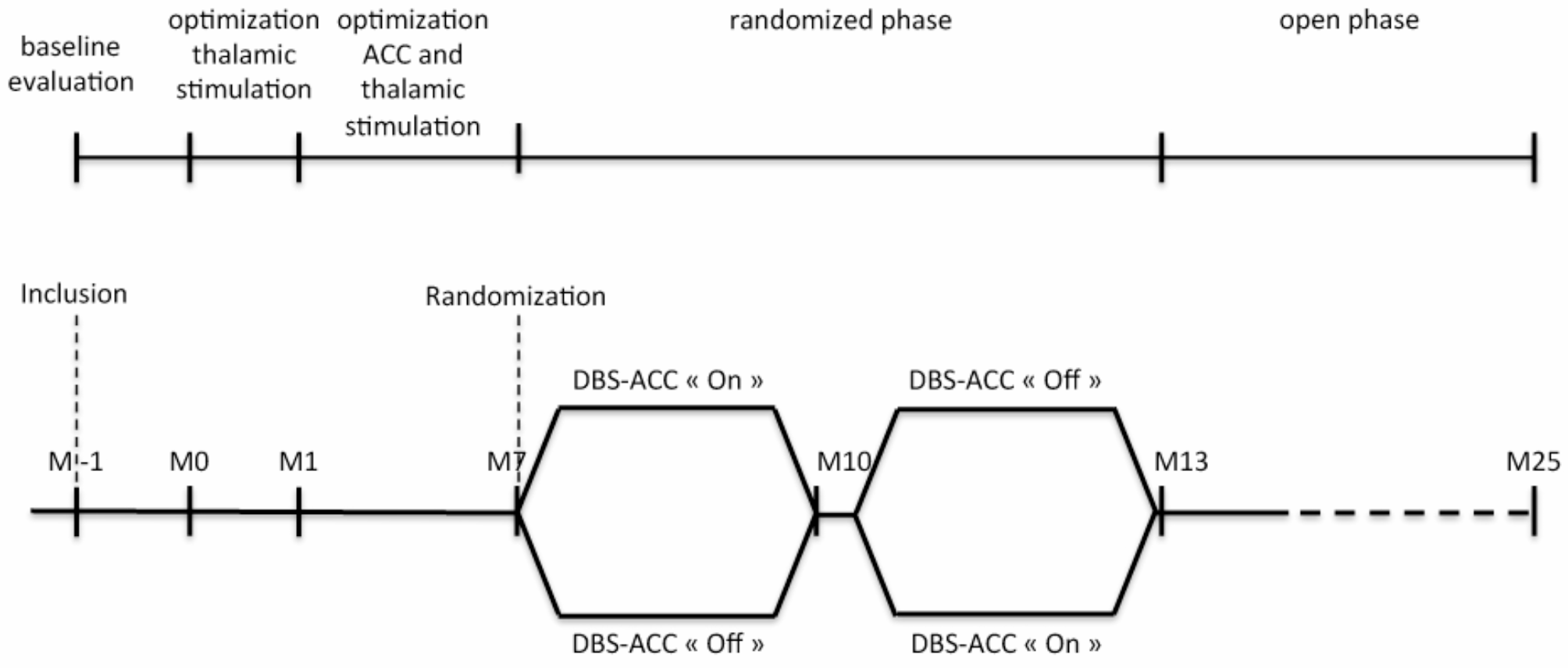
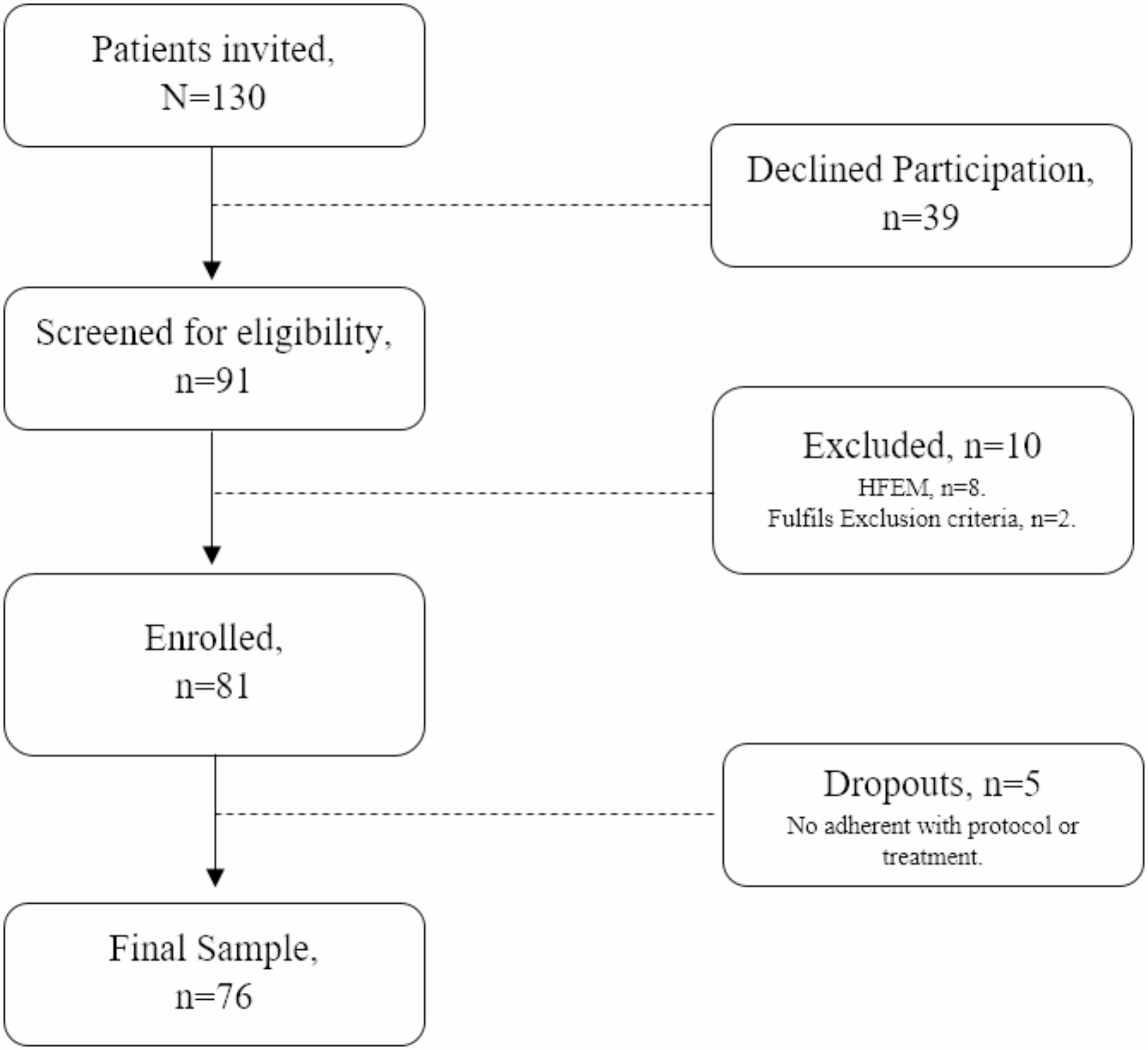
Sensory thalamic and ACC-DBS devices were implanted under local anesthesia in a single stage surgery. During the first month after surgery (M0-M1), only sensory thalamic-DBS was activated (Fig. 1). ACC-DBS was then activated one month after surgery (M1) and parameters settings were optimized during the next 3 months (M1-M4). Four months after surgery, all the patients were randomized in two 3 month-periods (separated by a 2-week wash-out period) organized in a cross-over design, comparing a DBS-ACC sequence on (“On”) and a DBS-ACC sequence off (“Off”). The patients and evaluating neurologists were blinded to the treatment periods and the ACC-stimulation parameters. This randomized period was followed by a 12-months open phase with ACC stimulation On.
Fig. 1
Study design. The study design consists of a 1-month pre-treatment evaluation phase, a phase of thalamic stimulation alone (1 month), then thalamic and anterior cingulate (ACC) stimulation (3 months), followed by a cross-over randomized phase comparing ACC stimulation “On” (3 months) and “Off” (3 months) periods, and then an open phase (12 months)
PatientsInclusion criteria were: adult patients (age 18–70 years old) suffering from chronic (duration > 1 year) unilateral NP (DN4 score ≥ 4/10), severe (VAS score ≥ 6/10 at 3 different evaluations during the year preceding inclusion), with high emotional impact (Hospital Anxiety and Depression scale sub-scores ≥ 10), considered as refractory to medication specific to neuropathic pain at sufficient doses and durations (including at least antiepileptics and antidepressants) and not sufficiently improved by rTMS or potentially relevant surgical solutions. Exclusion criteria were: cognitive impairment (MMSE score < 24), DSM-IV axis I psychiatric disorder, contra-indication to surgery, DBS, anesthesia or MRI.
Technical aspectsDetails concerning the surgical technique and stimulation parameters for thalamic- and ACC-DBS have been previously published [19]. One lead was implanted in the sensory thalamic nuclei contralateral to pain and two leads were implanted bilaterally and symmetrically in the ACC, and then connected to 2 generators. Sensory thalamic nuclei were targeted stereotactically based on the patient’s MRI and optimal position of the electrode was refined by intraoperative micro-electrode recordings and test stimulation to check that DBS-induced paresthesias were perceived in the painful body area. Stimulation intensity used for chronic stimulation was adapted to ensure that the stimulation-paresthesias were pleasant and felt in the painful region. The dorsal anterior cingulate was targeted on stereotactic MRI, according to the technique and location proposed by [10], approximately 20 mm posterior to the projection of the anterior tip of the frontal horn of the lateral ventricle. We chose to target the ACC bilaterally considering that, in chronic pain patients, ACC activity changes are bilateral [12] and that previous successful therapeutic procedures targeting the ACC, namely cingulotomies [13, 14] and DBS [9, 10, 17] were performed bilaterally. Stimulation of the ACC does not induce any perceptible feeling. The stimulation parameters were based on those used by [9, 10]. To avoid a “kindling” effect and the risk of epilepsy, the chronic stimulation was cyclic, alternating a 5-minute “On” phase and a 10-minute “Off” phase. The stimulation parameters were optimized, depending on the therapeutic or adverse effects observed, during the period between M1 and M4. The parameters found to be the most effective and best tolerated were used for the randomized phase.
EndpointsFeasibility was evaluated by the proportion of patients undergoing with success the process of surgical intervention, chronic stimulation and evaluation without serious adverse events. Safety profile and efficacy were evaluated 1 month before surgery and 1, 4, 7, 10, 22 months after by independent assessments performed by a neurosurgeon, a neurologist specialized in pain medicine, a psychiatrist and a neuropsychologist, the last three being blind from the randomization. Safety was evaluated by repeated general and neurological examination, psychiatric assessment, assessment of cognitive and affective functioning. The cognitive assessment consisted in several tests: the mini mental status (MMSE) [20] to evaluate global cognition, the French version of the Free and Cued Selective Reminding Test (FCSRT) [21] to assess episodic memory, the Digit Span WAIS-IV subtest to assess working memory, the Digit Symbol-Coding WAIS-IV subtest [22] to assess processing speed and the GREFEX battery [23] to assess executive functions, including the Trail Making Test (TMT), the Stroop test, the 6 element test, the Brixton test, the double task test, the modified card sorting test (MCST) and verbal fluencies. Assessment of affective functions was performed using Hospital Anxiety and Depression (HAD) scale [24] the Lille Apathy rating scale (LARS) [25], the revised version of “Reading the mind in the eyes” test [26] to assess theory of mind and the Facial Expressions of Emotion– Stimuli and Tests (FEEST) test [27] to assess emotion recognition.
DBS efficacy was evaluated using pain intensity on Visual Analogic Scale (VAS), Brief Pain Inventory [28], the QDSA questionnaire (French version of the Short-Form McGill Pain Questionnaire) [29] and quality of life improvement (EQ-5D-3 L health questionnaire) [30].
StatisticsTo assess the effects of DBS on cognition we performed paired samples Student’s t-tests on each raw score comparing Baseline to every other time of the study (Post-op, Thalamus only, Thalamus and ACC, Long term). A “p-value” and an “adjusted p-value” were computed using the Benjamini and Hochberg False Discovery Rate to minimize the type I error rate. As we could not identify a pattern in the missing data, no imputing method was used. The effect of DBS on functioning of cognitive domains (episodic memory, executive functions, processing speed, working memory and social cognition) was assessed by grouping relevant standardized scores and computing their mean values. Lastly, we calculated the variation of these scores between baseline and every other time of measure. This new score was called “delta-z”. Descriptive statistics were then computed. Given the design of the study and following appropriate statistical practice, we used linear mixed models (LMMs) [31]. We used linear mixed models with time as a fixed variable, subject as a random variable, and each cognitive variable to be predicted. We also modeled the effect of time and interindividual variability with a multivariate mixed linear model considering the mean standardized scores of the different cognitive domains (episodic memory, executive functions, processing speed, working memory and social cognition). When necessary for mixed linear modeling, mean imputation was performed.
Analyses were performed using the software R Statistical Software (v4.2.2; R Core Team, 2022) and the following R packages: lme4 (v.1.1.33; [32]), mice (v.3 0.16.0; [33]), rempsyc (v.0.1.2 ) [34], tidyverse (v.2.0.0; [35]), zoo (v.1.8.12; [36]).
Concerning the efficacy assessment, due to the small number of subjects in this study, statistical analysis was based on non- parametric tests. Results are presented as means (standard deviation [SD]) for quantitative variables. The scores comparisons between each visit and baseline were performed using the Wilcoxon signed- rank test. Alpha risk was set to 5% (α = 0.05). Statistical analysis was performed with EasyMedStat (version 3.27; www.easymedstat.com).
留言 (0)