
記住我

Women with a history of stroke with and without migraine had different stroke etiologies according to the TOAST classification. Of the women with stroke without migraine, around one quarter had a stroke of undetermined origin, whereas in the women with stroke and migraine, half had a stroke of undetermined origin. This suggests that women with migraine have a different stroke etiology than those without migraine. Our finding that women with stroke but no history of migraine were more frequently smokers than those with a history of migraine further supports the probability of a different underlying pathophysiological mechanism between women with stroke with and without migraine. Next, we found no increase in WMH volume due to migraine in women with stroke. Periventricular WMH volumes were higher in women with stroke and migraine than in those with MA alone.
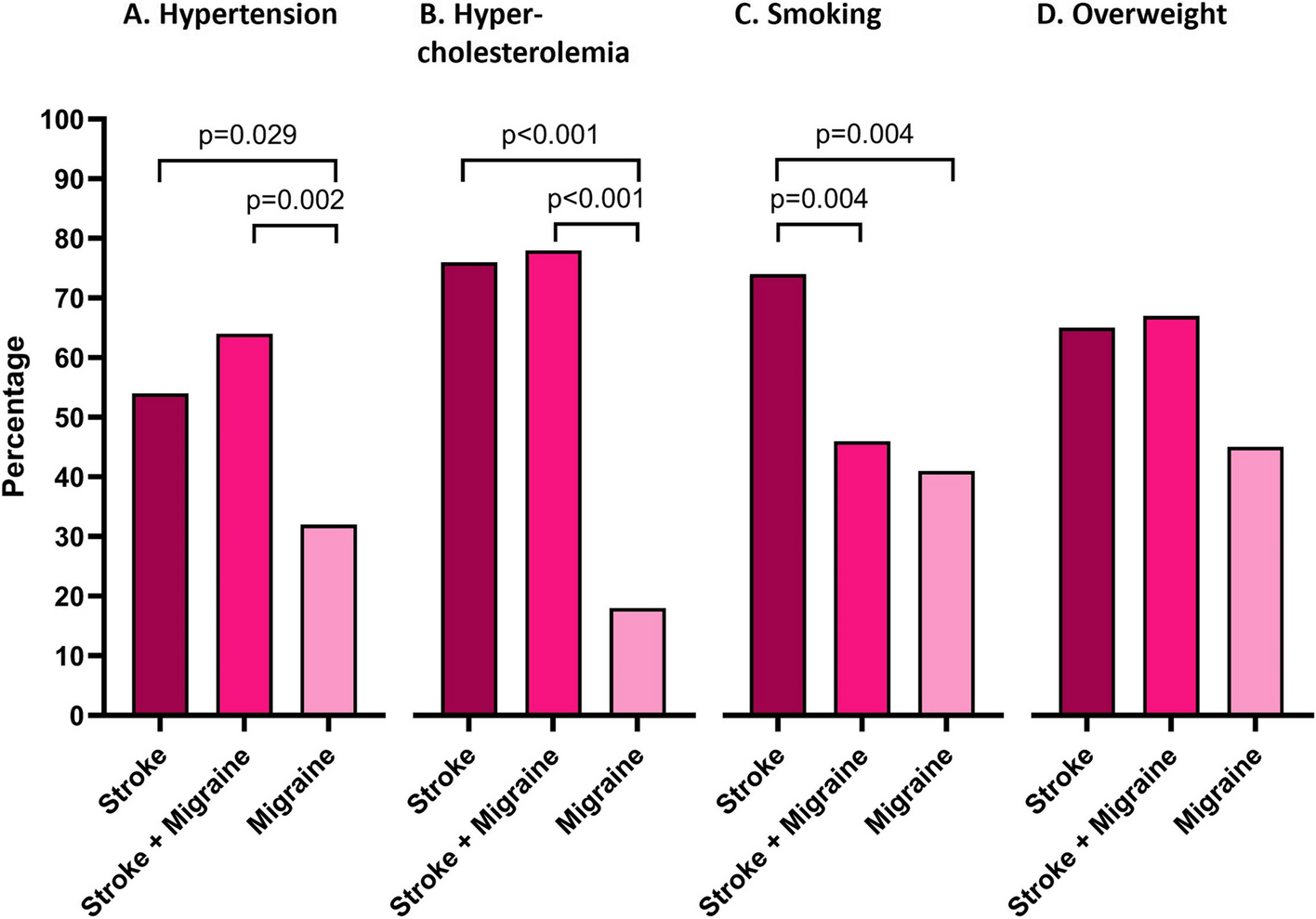
The precise mechanisms linking migraine and ischemic stroke are unclear. In this study, we demonstrate that the etiology leading to stroke in patients with and without migraine may differ. The absence of a causal factor for stroke is more common in patients with both migraine and stroke than in those with stroke alone, as supported by two prior studies [27, 28]. It is possible that these migraine patients experience strokes without requiring the involvement of other classic pathophysiological mechanisms, such as atherosclerosis or a cardio embolism. This is supported by earlier findings indicating that the increased risk of cerebrovascular disease (CVD) in migraine patients seems not to be due to (large artery) atherosclerosis caused by traditional cardiovascular risk factors [7, 29]. Our finding that women with stroke but no history of migraine were more frequently smokers than those with a history of migraine, further reinforces this hypothesis. Previous work also demonstrated that among patients with stroke and migraine fewer smoked compared to patients with stroke and no migraine (25.9% vs. 38.3%).[30] This is in line with a study on substance use in migraine patients, showing that patients with migraine are less likely to smoke, drink alcohol or use illicit drugs [31]. This of course does not prove that conventional risk factors do not play a role. In our study, women with stroke more often had a history of hypertension and hypercholesterolemia, than women with migraine alone, but there were no differences between women with stroke with and without migraine. Previous studies have found conflicting results on whether migraine increases the risk of hypertension, therefore the role it plays in the migraine stroke relationship remains controversial [32]. In general, there seems to be no clear dyslipidemia profile in patients with migraine [33, 34]. Still, sex-specific associations are indicative towards a less CVD-protective lipoprotein profile in women with migraine [33].
Several mechanisms have been implied to play a role in the relationship between migraine and stroke, such as CSD, endothelial dysfunction, altered cerebrovascular reactivity and neuroinflammation [9, 11]. Animal studies suggest that micro-emboli can trigger CSDs, potentially linking right-to-left cardiac shunting, often due to a patent foramen ovale (PFO), to migraine aura and stroke [35, 36]. CSD also affects ischemic stroke development, with peri-infarct depolarizations causing expansion of the infarct core. Transgenic hemiplegic migraine mouse models with experimentally induced stroke had larger infarcts due to a higher propensity for peri-infarct depolarizations [37]. While migraine preventive treatment protected mice from ischemic injury, clinical studies have shown inconsistent results [38]. In a large population based study the increase in WMH in migraine subjects was independent on whether subjects had active or non-active migraine and frequency of attacks [16].
Endothelial dysfunction is another suggested shared mechanism between migraine and stroke, involving reduced cerebrovascular reactivity and markers for endothelium activation, hypercoagulability, and inflammation [39]. Enhanced platelet aggregation in migraine patients suggests a potential link controlled by the endothelium [40]. Reduced vascular reactivity might partly explain the connection between migraine and stroke, as evidenced by increased arterial stiffness and impaired cerebral vasodilator function [41].
Even though the absolute risk for developing stroke remains low for (young) women with migraine, there are implications for clinical practice [2]. The use of oral contraceptives increases the relative risk for stroke, especially in patients with MA [2]. This relative risk is further increased to a 35 times in women with MA who use oral contraceptives and also smoke [6]. Therefore, combined hormonal contraceptives are not recommended in women with MA and migraine patients who smoke. In the past, there have been worries that acute medications to treat migraine attacks, such as triptans, might increase the risk of stroke, because of their vasoconstrictive properties. A novel study found a short-term increased risk in myocardial infarction and ischemic stroke after triptan initiation, although the absolute risk remained very low in these patients [42]. However, previous clinical studies have shown that triptan use is not associated with an increase in cardiovascular events and, based on expert opinion, triptan use is considered safe in many countries [43]. Recently, selective 5HT1F receptor agonists (ditans) have been developed that do not cause vasoconstriction, as such they may be even better suited for stroke patients [44]. There are some safety concerns related to the use of calcitonin gene related peptide (CGRP) monoclonal antibodies and small molecule CGRP antagonists in migraine patients with stroke, because of the blockage of vasodilation as an escape response [45]. There is one case report of a 41-year old woman with MO who developed a stroke after the first dose of a CGRP receptor blocker [46]. Furthermore, real world data studies showed an increase in mean blood pressure in patients treated with anti-CGRP (receptor) antibodies (compared to control migraine patients), with some patients requiring antihypertensive treatment [47, 48]. Therefore, use of anti-CGRP (receptor) antibodies is not recommended in stroke patients until the long-term safety has been established.
Our study comes with some limitations. Firstly, the sample size of all groups is relatively small and the overall WMH volumes were low, as such, subtle differences in WMH volume between patients with and without migraine and stroke might have been missed. Furthermore, as we performed a clinic based study, our results might possibly not be generalizable to all populations. This, however, led to rich medical data and a clearly defined homogeneous population. Next, based on available data, we used the TOAST classification to divide stroke in subgroups, however newer classification systems have been proposed that might be more specific [49]. We were also unable to look into differences between migraine types (MA and MO) and migraine severity. While we aimed to determine if migraine itself let to an increased WMH volume in stroke patients, as both migraine with aura and migraine without aura are at risk of sub-clinical brain lesions, future efforts should focus on whether migraine with aura might lead to a subtle increase in WMH volume that we might have missed by also including stroke patients with migraine without aura. The group of women with a history of migraine and stroke consisted of both MA and MO patients, whereas the migraine only group consisted solely of patients with MA (although it should be noted that most MA patients also experience MO attacks). As previously mentioned, MA patients without stroke were included as effect size was expected to be larger in this group compared to MO. If a difference was found in WMH volume, this would then logically also be expected to exist between stroke patients with migraine and MO patients. Lastly, the interval between stroke and the study visit was not standardized, resulting in considerable variability. Nonetheless, there was no significant difference in median time between stroke and study visit between the two stroke groups.
Strengths of our study are the use of semi-automated software on high-quality 3T MRI scans for the assessment of WMH, leading to precise estimates of volumes (Fig. 4). Moreover, we used a validated and well-defined national cohort of migraine patients, and next to including stroke patients from the LUMC, we included women from all over the Netherlands through online advertisement, increasing the generalizability of the study population [19]. Furthermore, the migraine diagnosis was assessed and validated by a headache specialist (GT), and the stroke diagnosis by a stroke specialist (MW). Lastly, to our knowledge, this is the first study to extensively study the presence and amount of WMH in women with stroke with and without a history of migraine.
Fig. 4
Example of white matter hyperintensities (WMH) on 3D fluid-attenuated inversion recovery (FLAIR) images of three women: A a woman with migraine with aura, the arrow marks a deep WMH; B a woman with a history of stroke, the arrow marks a deep WMH, the asterisks mark the area affected by the stroke; C a woman with a history of migraine and stroke (stroke lesions not depicted on image)
留言 (0)