
記住我
Anxiety disorders represent a significant and pervasive mental health issue globally, affecting millions of individuals and imposing a considerable burden on society. Empirical data reveals that anxiety disorders are among the most prevalent mental health conditions, with estimates suggesting that they affect around 18% of the global population (1). This high prevalence, combined with their chronic nature and frequent comorbidity with other mental health conditions, has led the World Health Organization (WHO) to rank anxiety disorders as the ninth leading cause of disability worldwide (2). Anxiety, characterized by an unpleasant emotional state with experiential, physiological, and behavioral components, serves as a vital warning mechanism for individuals (3). As defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), anxiety encompasses a range of diagnoses, including panic disorder, agoraphobia, generalized anxiety disorder, post-traumatic stress disorder (PTSD), social phobia, acute stress disorder, obsessive-compulsive disorder, and disorders related to medical conditions or substance use (4). Manifesting in symptoms such as sweating, chills, trembling, increased heart rate, hyperventilation, and a sense of impending doom, anxiety disorders can severely impact an individual’s quality of life (5).
Furthermore, research has demonstrated that persistent anxiety is associated with an elevated risk of cardiovascular diseases, with a risk ratio of 1.5 (6). In addition to cardiovascular diseases, anxiety has been linked to an increased risk of developing other physical illnesses, such as stroke, diabetes, arthritis, and lung diseases, compared to the general population (7). The mechanisms contributing to this higher comorbidity risk in populations with anxiety disorders may include unhealthy lifestyles, poor treatment adherence, and dysregulation of psychobiological stress systems. Therefore, early integration of physical health concerns into the treatment of anxiety disorders is crucial. Additionally, anxiety disorders can lead to unstable interpersonal relationships, functional impairment, and increased workplace absenteeism, resulting in substantial economic losses (8). Given these alarming statistics and the multifaceted impact of anxiety disorders, it is imperative to explore effective interventions, such as High-Intensity Interval Training (HIIT), to address this pressing public health issue.Reducing the substantial burden of disease caused by anxiety disorders, both for individuals and globally, can be most effectively achieved through timely and accurate disease detection, along with the administration of adequate treatment and the scaling up of interventions when necessary. Worldwide, the treatment rate for anxiety symptoms remains low, a challenge that is particularly pronounced in low-income countries but continues to be a pressing issue in high-income countries as well (9).
As mental health concerns like anxiety rise, while prescription medications and psychotherapy remain essential, current studies indicate that increased reliance on exercise, such as High-Intensity Interval Training (HIIT), can alleviate negative moods and reduce healthcare costs (10). HIIT’s effectiveness across various health parameters is supported by empirical evidence (11), and theoretical frameworks provide insights into its mechanisms.Theoretically, HIIT aligns with Social Cognitive Theory (SCT), which suggests that successful engagement in challenging activities like HIIT can enhance self-efficacy, leading to improved mental health outcomes, including reduced anxiety (12). The Theory of Planned Behavior (TPB) indicates that HIIT’s structured and time-efficient nature may enhance perceived behavioral control, promoting adherence and long-term engagement (13).Empirically, HIIT involves intensities eliciting ≥80-100% of peak heart rate, with “all-out” Sprint Interval Training (SIT) exceeding maximal oxygen uptake (14). Originally for endurance athletes, HIIT now benefits the general population, including previously sedentary individuals (15). Studies show HIIT significantly improves anxiety symptoms, especially in those with lower baseline anxiety levels (16), highlighting its potential as a therapeutic intervention for mental health.
Exercise training has been shown to effectively improve mood disorders in both humans and rodents, with recent studies indicating that exercise can ameliorate chronic stress-induced anxiety in mice by modulating RNA N6-methyladenosine (m6A) levels (17). Despite extensive literature on general exercise therapy for anxiety and depression (18), research specifically on High-Intensity Interval Training (HIIT) remains in its early stages, with only a limited number of studies exploring its effectiveness in alleviating anxiety symptoms. To address this gap, this scoping review aims to summarize existing systematic reviews related to HIIT and anxiety, understand its current role in anxiety research, identify gaps, and determine future research directions. By enhancing HIIT interventions for anxiety patients, this review seeks to guide clinical practice. The paper will introduce the research question, outline the scoping review methodology, compile and analyze relevant literature, and interpret findings within the broader context of mental health research, suggesting practical implications and avenues for future research. This structured approach ensures the research question is grounded in current knowledge while paving the way for innovative advancements in the field.
2 Materials and methodsThis review has been carried out in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (19) and PRISMA 2020 checklist (Supplementary File 1).
2.1 Research designThis scoping review will employ a systematic and rigorous methodology to synthesize the existing evidence on the impact of High-Intensity Interval Training (HIIT) on anxiety. The review will commence with an extensive search of electronic databases, including PubMed, Web of Science, Scopus, and Cochrane Library, to identify relevant studies. The search strategy will be developed using a combination of keywords related to HIIT, anxiety, and their interrelationship. Additionally, reference lists of retrieved articles and gray literature sources will be screened to ensure comprehensive coverage. Studies included in the review will be screened based on predefined inclusion and exclusion criteria, focusing on original research articles that investigate the relationship between HIIT and anxiety in humans. Data extraction will involve summarizing key characteristics of each study, including population demographics, study design, HIIT protocols, anxiety assessment tools, and main findings. The extracted data will be synthesized narratively, highlighting key trends and findings across studies. Furthermore, the review will examine the specific effects of HIIT on anxiety across different populations and settings, and explore potential mechanisms underlying the relationship between HIIT and anxiety. Finally, the review will identify research gaps and suggest future directions for research in this area, contributing to a more nuanced understanding of the impact of HIIT on anxiety and informing evidence-based practice and policy recommendations.
2.2 Search strategyTo identify relevant studies, we conducted an extensive search of the following electronic databases: PubMed, Web of Science, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL), as well as Chinese databases including CNKI (China National Knowledge Infrastructure), Wanfang Data, and VIP (Chongqing VIP Information). These databases were chosen to cover a broad spectrum of medical, psychological, and scientific literature. The search covered all available years from the inception of each database up to September 25, 2024, ensuring the inclusion of the most recent research.A combination of controlled MeSH terms and free text were used as descriptors, which were combined with the Boolean operators ‘AND’ and ‘OR’The following search terms were used: (((((anxiety [Title/Abstract]) OR (angst [Title/Abstract])) OR (nervousness [Title/Abstract])) OR (anxious [Title/Abstract])) AND (High Intensity Interval Training [Title/Abstract])) OR (HIIT [Title/Abstract]) OR (repeated sprint training [Title/Abstract]) OR (sprint interval training [Title/Abstract]) OR (High-Intensity Intermittent Exercise [Title/Abstract]) (Supplementary File 2).
To carry out this review, a protocol was created and registered in PROSPERO (international prospective register of systematic reviews) under the number: CRD4202230342.
2.3 Inclusion criteriaInclusion criteria were determined according to the PCC (Population, Concept, Context) principle: (1) Participants: Studies were included if they involved human subjects who received High-Intensity Interval Training (HIIT) as a therapeutic intervention aimed at improving anxiety (20). (2) Concept: Studies that involve high-intensity exercises interspersed with recovery periods, including those defined as HIIT or Sprint Interval Training (SIT). High-intensity exercise is defined as achieving >85% of VO2peak, reaching 85% of HRmax, or utilizing equivalent perceived exertion-based methods. Studies must adopt an intervention design with a training period lasting >1 week and should exclusively focus on HIIT (21). Additionally, studies should include measures related to any of the following outcomes: (i) muscle function (strength or power), (ii) muscle mass, or (iii) physical performance (22). (3) Context: Studies conducted in any type of setting (e.g., laboratory, private clinic, rehabilitation center, hospital) where anxiety is the primary outcome measure were selected based on predefined criteria including randomized controlled trials (RCTs), cohort studies, and quasi-experimental designs (23). Physical improvements from HIIT enhance self-efficacy, body image, and confidence in daily activities, while also promoting better sleep and mood, all of which can positively impact anxiety levels. These outcomes serve as important secondary markers, providing insights into the broader mental health benefits and long-term effectiveness of HIIT (24–27).
2.4 Exclusion criteria(1) Studies that have not undergone full peer review (e.g., conference proceedings, posters, published abstracts, non-peer-reviewed articles, proposed studies, theses, dissertations, reviews, commentaries, debates). (2) Duplicates of published literature. (3) Studies for which the full text is not available. (4) Animal experiments, reviews, letters to the editor, and similar publications. (5) Manuscripts written in languages other than English. Exclude studies where randomization is not applied to a control group, such as studies comparing two experimental groups without a control group. (6) Studies involving animal models (e.g., rodent models). (7) Studies where HIIT is combined with other interventions (e.g., cognitive-behavioral therapy, pharmacotherapy). No language restrictions were applied to ensure that potentially relevant studies were not excluded due to the language of publication. Only full-text articles that met the eligibility criteria were considered for inclusion.
2.5 Data itemsData extracted from each study included sample size, group descriptions, study design, analytical methods, and outcome data. Methodological quality was assessed using a modified 0–10 point PEDro scale (16). Primary outcome variables were defined as pre- and post-intervention self-report questionnaires [Beck Anxiety Inventory (BAI), State-Trait Anxiety Inventory (STAI), Hospital Anxiety and Depression Scale (HADS)], clinical assessment tools [Clinical Global Impression (CGI), Structured Clinical Interview for DSM Disorders (SCID)], physiological indicators (heart rate variability (HRV), galvanic skin response (GSR), cortisol levels), and behavioral indicators (task performance, self-reported behavioral changes). Due to the heterogeneity in inclusion criteria, interventions, assessment tools, and outcomes, a meta-analysis was not deemed appropriate. The reliability and validity of the scales used in this scoping review have been rigorously tested in previous studies. For instance, the Beck Anxiety Inventory (BAI), a 21-item self-report questionnaire designed to measure the severity of anxiety symptoms, has demonstrated high internal consistency (Cronbach’s α typically ranging from 0.90 to 0.94) and good test-retest reliability (28). The BAI is widely recognized for its strong psychometric properties and has been validated across various populations (29). Similarly, the State-Trait Anxiety Inventory (STAI), which includes two separate 20-item subscales for measuring state anxiety (STAI-S) and trait anxiety (STAI-T), has shown excellent reliability and validity in numerous studies (30). The STAI-S assesses transitory anxiety levels related to specific situations, while the STAI-T measures more stable, long-term anxiety tendencies. The Hospital Anxiety and Depression Scale (HADS), a 14-item scale with two subscales for anxiety and depression, has also been extensively validated (31). It is commonly used in clinical settings and has demonstrated good sensitivity and specificity for detecting anxiety and depressive disorders. For clinical assessment tools, the Clinical Global Impression (CGI) scale, which consists of three subscales—Severity, Improvement, and Efficacy Index—has been widely used and validated in psychiatric research (32). The CGI provides a global assessment of symptom severity and treatment response by clinicians. The Structured Clinical Interview for DSM Disorders (SCID) is a comprehensive diagnostic tool that has undergone rigorous testing for both reliability and validity (33). SCID is used to diagnose mental disorders according to DSM criteria and is considered a gold standard in clinical assessments.
2.6 Data extractionTwo authors independently conducted the literature search. After completing the search of each database and retrieving the papers, all studies were downloaded into a single reference list and imported into EndNote X9 software to remove duplicates. Titles and abstracts were then screened to determine if they met the inclusion criteria, with only studies involving HIIT selected for full-text retrieval. Subsequently, the two reviewers read and coded all included articles using the PEDro scale (34). Following this, the full texts were thoroughly evaluated against the inclusion and exclusion criteria, with final confirmation provided by the first author and the corresponding author. After this quality assessment, the same reviewers read and coded each study, evaluating the following moderators: study design [randomized controlled trial (RCT), controlled trial (CT), or uncontrolled trial (UCT)], whether HIIT was used alone or in combination, and outcome variables. Additionally, detailed participant descriptions and training program variables were extracted. Any discrepancies between reviewers were resolved during consensus meetings, with the consultation of a third researcher when necessary, to finalize the list of studies meeting the criteria. Data extraction was performed using a standardized form and cross-checked for accuracy (see the Data extraction flow diagram in Figure 1).
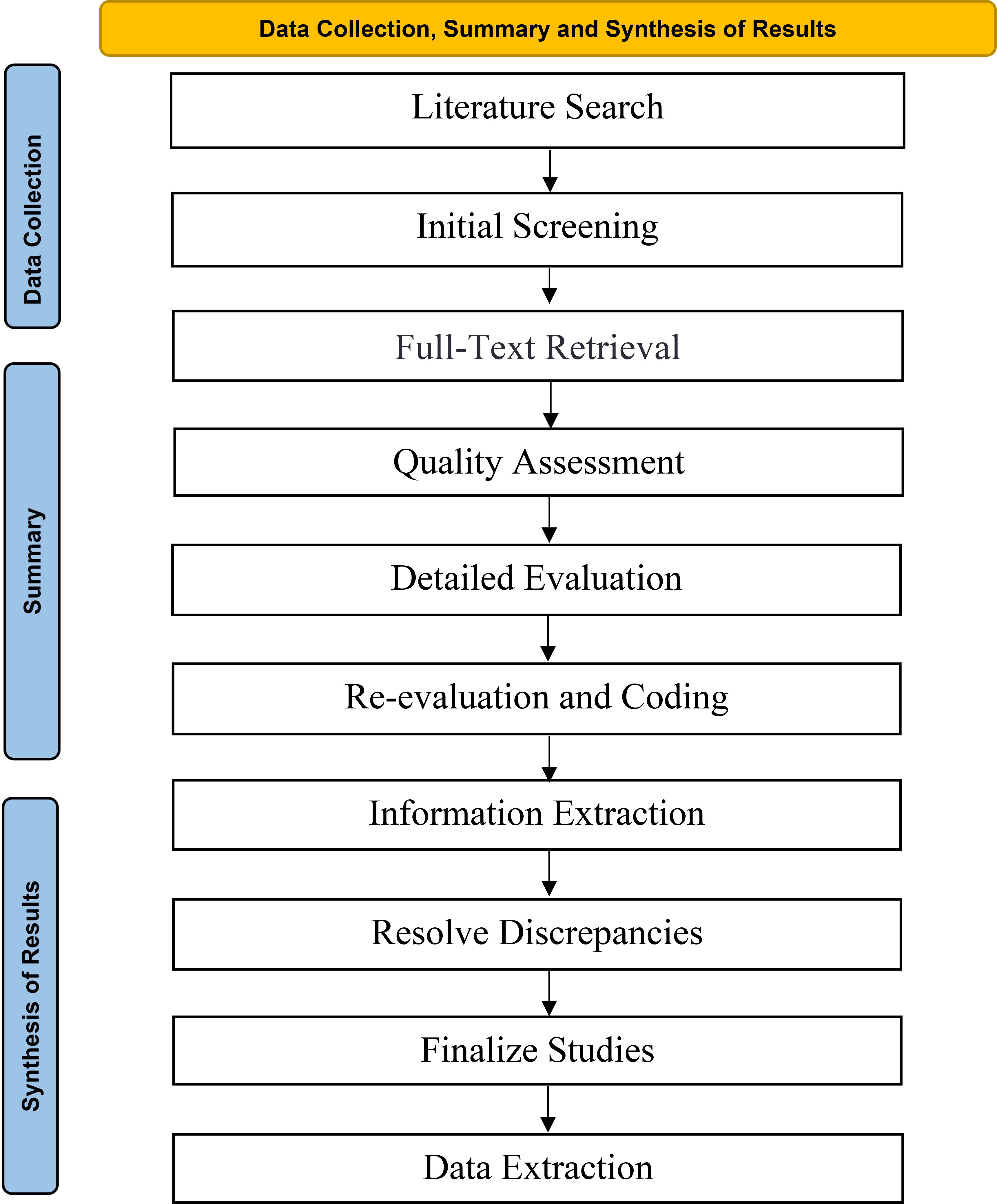
Figure 1. Data collection, summary and synthesis of results flow diagram.
3 Results3.1 Results of the literature searchThe search strategy identified 541 records across four electronic databases. After removing duplicates, 416 records remained. Of these, 302 records were excluded based on title and abstract screening. The full texts of the remaining 115 articles were assessed, and ultimately, 16 studies meeting the inclusion criteria were included (see the PRISMA flow diagram in Figure 2).
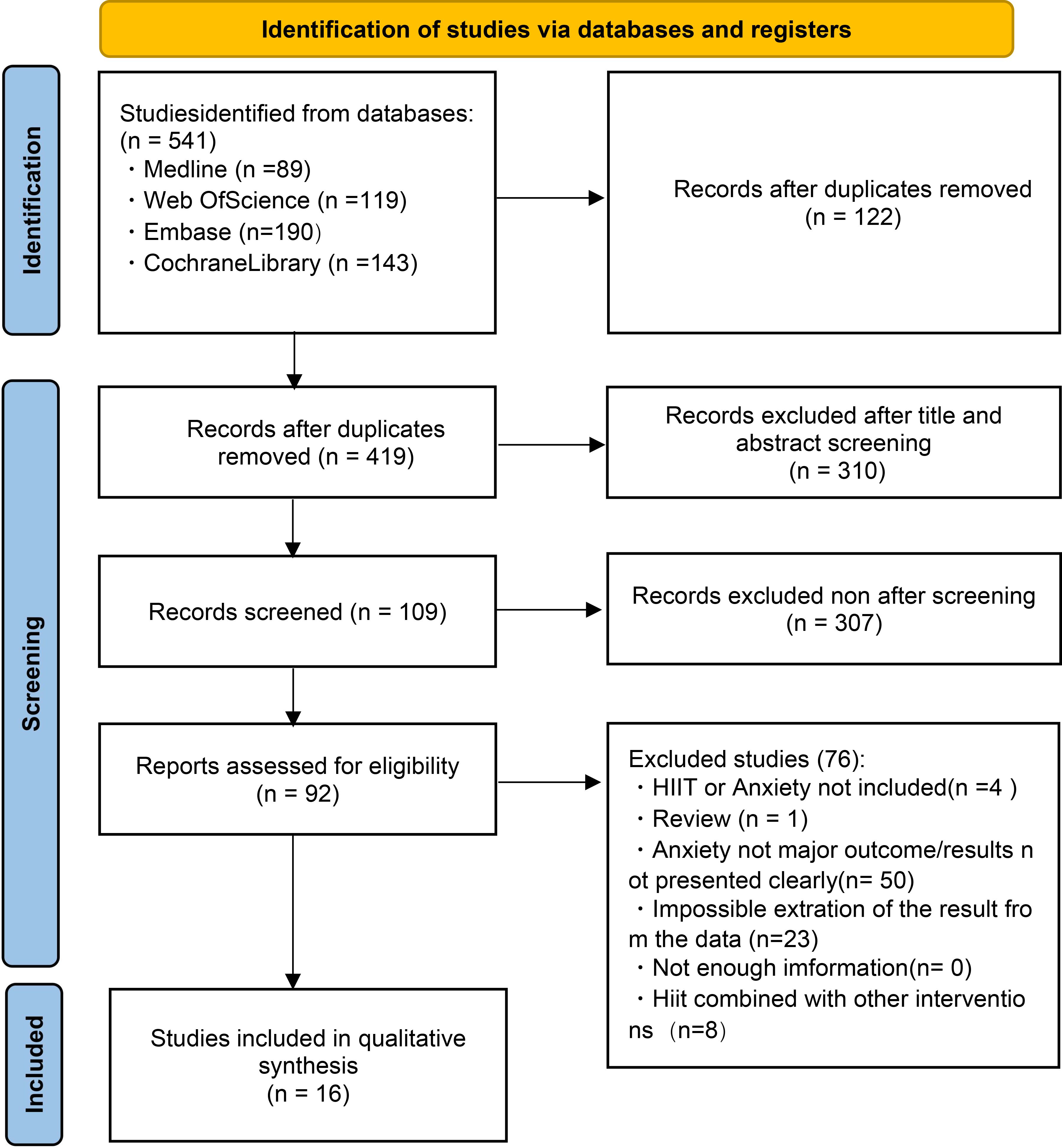
Figure 2. Flow diagram of trials selection process.
3.2 Characteristics of included studiesThe characteristics of these studies are outlined in Table 1. All included studies were published between 2005 and 2024. Specifically, publications were made in 2005 (n = 1), 2018 (n = 2), 2019 (n = 2), 2020 (n = 4), 2021 (n = 2), 2022 (n = 2), 2023 (n = 2), and 2024 (n = 1). Studies were conducted in eleven different countries or regions, with one study from Spain, two studies from Brazil, one study from Ireland, one study from the U.S.A., three studies from Canada, one study from Australia, one study from China, two studies from Germany, two studies from Tunisia, one study from Italy, and one study from Taiwan. And Canada contributed the most studies (n = 3). Four studies originated from Europe, two studies came from North America, two studies were from Asia, one study was from Oceania, one study was from South America, and one study was from Africa. The total sample size across all studies was 570 participants, with individual study participant numbers ranging from 12 to 67. Three studies included only female participants, five studies included only male participants, and eight studies included both male and female participants. The samples comprised various populations, including healthy subjects (n = 6) (35, 36, 38, 41, 44, 49), overweight males (n = 1) (37), prostate cancer patients (n = 1) (39), sedentary individuals (n = 1) (40), asthma patients (n = 1) (42), women with polycystic ovary syndrome (PCOS) (n = 1) (43), panic disorder patients (n = 1) (45), generalized anxiety disorder patients (n = 1) (46), soccer players (n = 2) (47, 48), and patients attending a psychiatric day care unit (n = 1) (50). Three studies involved participants diagnosed with anxiety and related affective disorders (45, 46, 50). Most studies adopted a randomized controlled trial (RCT) design (n = 10), while others included observational cohort studies (n = 3), pilot studies (n = 1), longitudinal studies (n = 1), and prospective studies (n = 1).

Table 1. Characteristics of included studies.
3.3 Intervention characteristicsIn the 16 HIIT protocols applied in the reviewed studies, 12 (75%) were classified as HIIT, 3 (18.8%) were classified as SIT, and 1 (6.3%) was classified as aerobic and speed training. The classification of these protocols is based on the definitions and criteria explicitly described by the authors within their respective studies. There was considerable variation among the interval training protocols; for example, the duration and intensity of warm-up, cool-down, work intervals, and rest periods differed significantly. Among the sixteen studies, the warm-up protocols prior to initiating HIIT varied as follows: five studies included a 5-minute warm-up; two studies implemented a 2-minute warm-up; one study conducted a 3-minute warm-up; one study performed a 10-minute warm-up; and one study carried out a 15-minute warm-up. Notably, six studies did not provide any description of their warm-up procedures. Regarding training intervals, two studies set specific exercise distances as their training targets: one aimed for 200 meters (37) and the other for 240 meters (48). The remaining fourteen studies targeted specific training durations. Among these, three studies had single-session training durations of less than 30 seconds (16, 38, 41), while six studies set a single-session training duration of 1 minute.
Following each bout of high-intensity exercise, ten studies incorporated rest intervals of 1 minute or less, one study designed a 2-minute rest interval, one study specified a 3-minute rest interval, and another study implemented a 4-minute rest interval. One additional study also used a 1-minute rest interval, whereas one study did not specify the duration of rest intervals.The most commonly reported interval training protocol was the HIIT scheme, which included a 5-minute warm-up, 1 minute of high-intensity exercise, followed by a 60-second recovery period (n = 4).
Regarding the mode of exercise in the intervention groups, 7 studies used cycle ergometers, 1 study used treadmills, 2 studies involved bodyweight resistance training, and 5 studies included repeated running or sprint training. The articles reported psychological and psychiatric outcome assessments, primarily focusing on anxiety. The training durations mostly ranged from 1 to 8 weeks, with 6 or 8 weeks being the most common intervention lengths. The frequency of exercise was predominantly three times per week. The control groups typically engaged in moderate aerobic exercise or received no specific intervention. Six studies reported 100% adherence among their participants, indicating that all participants in these studies strictly followed the designated protocols throughout the intervention period.
3.4 Measurement of anxietyThe primary outcome measure was anxiety level. All studies used a variety of assessment tools to evaluate anxiety levels, including the State-Trait Anxiety Inventory (STAI) (n=3), Beck Anxiety Inventory (BAI) (n=4), Memorial Anxiety Scale for Prostate Cancer (n=1), Anxiety Sensitivity Index-3 (ASI-3) (n=1), Depression, Anxiety, and Stress Scale (DASS-21) (n=2), Panic and Agoraphobia Scale (PAS) (n=1), Clinical Global Impression (CGI) (n=1), Hamilton Anxiety Rating Scale (n=1), Anxiety Control Questionnaire-Revised (ACQ-R) (n=1), and Competitive State Anxiety Inventory (CSAI-2) (n=2). Overall, the Beck Anxiety Inventory (BAI) (28) was the most commonly used measure.
Kang’s study assessed PCa-specific anxiety by the Memorial Anxiety Scale for Prostate Cancer (MAX-PC), which consists of a total score and 3 subscales assessing PCa anxiety, prostate specific antigen (PSA)-related anxiety and fear of recurrence (39). In their respective studies, Mason and O’Neill chose the Anxiety Sensitivity Index-3 (ASI-3) as the measurement tool for undergraduate students and community members, as well as for individuals with asthma. The reason for this choice may be that the ASI-3 can directly measure the core variable of anxiety sensitivity rather than general anxiety levels. This allows for a better understanding of how Sprint Interval Training (SIT) and Moderate Intensity Continuous Training (MICT) impact anxiety sensitivity. Additionally, the ASI-3 provides sufficient sensitivity to detect the effects of the interventions, thereby offering robust support for or against the study hypotheses.
Positive effect studies demonstrated significant reductions in anxiety sensitivity and asthma-specific anxiety following the six-week HIIT intervention compared to the control groups. These improvements were evident across various age groups, genders, and health statuses. In contrast, studies with negative results did not show a significant difference in anxiety sensitivity or asthma-specific anxiety between the HIIT group and the control group.
Among the 16 included studies, 12 reported that HIIT could improve anxiety levels in participants. One study indicated that three weeks of SIT could enhance anxiety and worry in young adult males. The training protocol included 4 to 6 maximal 30-second cycling sprints, with each sprint followed by 4 minutes of active recovery. Participants began the session with a 5-minute warm-up and ended with a 3-minute cool-down period (38).
Twelve weeks of HIIT reduced prostate cancer-specific anxiety (total score and fear of progression), hormonal dysfunction, and general psychosocial outcomes (stress, fatigue, and self-esteem), primarily attributed to a moderate to large reduction in fear of cancer progression (d = -0.67). The training protocol included 5-minute warm-up, followed by 2 to 8 cycles of 2-minute high-intensity walking or jogging and 2-minute active recovery, concluding with a 5-minute cooldown and 5 minutes of lower body muscle stretching (39).
Another study demonstrated that six weeks of HIIT (35) reduced anxiety, stress, and depression while increasing resilience in the general population during COVID-19 confinement, potentially linked to the activation of endogenous opioid substances that alleviate stress (51). O’Neill’s study (42) showed that a six-week HIIT intervention reduced anxiety sensitivity and asthma-specific anxiety in adults with subclinical anxiety levels, with these reductions being independent of gender, supporting the prescription of high-intensity interval training. For patients with existing anxiety symptoms, the intervention effects of HIIT were twice as large compared to low-intensity training, suggesting it could serve as a first-line complementary treatment for this condition (46).
Four studies indicated that HIIT did not improve anxiety. One study found that moderate-intensity continuous training (MICT) could reduce anxiety levels in middle-aged overweight men, while the anxiety levels in the HIIT group showed no significant changes. The observed differences in anxiety reduction between MICT and HIIT groups may be attributed to variations in perceived exertion, exercise adherence, physiological adaptations, individual variability, and measurement sensitivity. These factors highlight the importance of considering both the type and intensity of exercise when designing interventions aimed at improving mental health outcomes in specific populations.
Additionally, De Sousa (37) and Lucibello (40) noted that nine weeks of HIIT training did not reduce anxiety symptoms, depressive symptoms, or inflammatory states. From the perspective of participant characteristics, individual differences in baseline health status, mental health condition, and personal preferences may influence each participant’s response to different types of training.
Middle-aged overweight men might benefit more from the steady and manageable challenge of Moderate Intensity Continuous Training (MICT) compared to the intense demands of High-Intensity Interval Training (HIIT) (52, 53).
For people with asthma, anxiety symptom severity moderated cardiorespiratory improvements from HIIT such that individuals with low anxiety at baseline experienced greater improvements than those with higher anxiety. This points to a novel non-responder phenotype based on anxiety status.
Despite Lucibello’s 9-week High-Intensity Interval Training (HIIT) program for young adults not reducing symptoms of anxiety, depression, or inflammation status, the severity of anxiety symptoms can moderate improvements in cardiorespiratory fitness from HIIT. Specifically, individuals with lower baseline anxiety levels exhibited greater improvements compared to those with higher anxiety levels. This points to a novel non-responder phenotype based on anxiety status (40).
A randomized controlled trial examining the impact of HIIT on students’ psychological states during the COVID-19 pandemic indicated that both HIIT and moderate-intensity training (MIT) could reduce stress, anxiety, and depression levels, while also enhancing psychological resilience. However, the improvement in depression appeared to be greater in the HIIT group compared to the MIT group.
These variations highlight the need for further investigation into the factors influencing the efficacy of HIIT interventions, such as individual differences in exercise tolerance, genetic backgrounds, lifestyle, and psychological states.
The observed variations in response to High-Intensity Interval Training (HIIT) among participants highlight the need for a deeper understanding of several influencing factors. These variations can be attributed to individual differences in exercise tolerance, genetic backgrounds, lifestyle factors, and psychological states (54). Participants with higher baseline fitness levels may tolerate and benefit more from HIIT compared to those with lower fitness levels. Genetic factors play a crucial role in determining how individuals respond to exercise. Some individuals may have genetic profiles that predispose them to better adaptation to high-intensity training, while others might not respond as positively (55).
Lifestyle encompasses various aspects such as diet, sleep patterns, alcohol consumption, smoking status, and overall physical activity levels outside of the intervention (56). Participants with healthier lifestyles—such as balanced diets, adequate sleep, and regular physical activity—may see more pronounced benefits from HIIT. Psychological states include mental health conditions, stress levels, motivation, and personal attitudes towards exercise. Individuals with pre-existing anxiety or depressive symptoms might find it more challenging to engage fully in HIIT due to increased psychological stress (20).
4 Discussion4.1 Summary of findingsThis scoping review investigated the application of HIIT in managing anxiety, summarizing findings from 16 eligible studies that reported outcomes related to anxiety associated with HIIT. The review provides a comprehensive perspective, aiding researchers and clinicians in understanding the potential of HIIT for anxiety management.While the results of the reviewed studies were mixed, a synthesis of multiple relevant studies revealed the value of HIIT in reducing anxiety levels, some studies show no significant effects. Most studies reported HIIT significantly decreased anxiety scores, with reductions averaging 7 to 10 points on standardized measurement tools such as the Beck Anxiety Inventory (BAI) and State-Trait Anxiety Inventory (STAI), indicating clinically meaningful changes. Improvements in at least one measure of muscle function or physical performance following HIIT interventions, indicating that HIIT may benefit not only mental health but also physical function. Despite the high intensity of HIIT, overall adherence was good, with an average attendance rate of 85%, reflecting the feasibility of HIIT as an intervention method. Additionally, this study focused on the impact of HIIT alone on anxiety and did not include other interventions combined with HIIT. This choice emphasizes assessing the potential therapeutic effects of HIIT itself on anxiety symptoms rather than the effects of combined interventions (57), which might have led to an underestimation of the potential benefits of integrated intervention strategies.
Some studies indicate that short-term HIIT programs, such as those lasting 4-6 weeks, can improve cardiovascular health and metabolic markers (48). However, the positive effects on mental health might require a longer duration to become evident (58). In contrast, HIIT programs that span several months may have a more pronounced positive impact on mental well-being (59). A defining characteristic of HIIT is its high-intensity interval pattern; however, the standard for what constitutes “high-intensity” varies across studies. Generally, HIIT intensity ranges from 80% to 95% of maximum heart rate. In this study, HIIT intensity was set above 85% of maximum heart rate, which falls within the typical range for high-intensity exercise (60). High-intensity training may lead to higher physiological stress responses, potentially affecting psychological states. However, it could also cause excessive stress for some individuals, which might be counterproductive to mental health (61). In comparison, moderate-intensity HIIT may be more suitable for beginners and easier to sustain (59). Appropriately adjusting the intensity of training may enhance the effectiveness of the regimen.
HIIT may influence anxiety through mechanisms such as endorphin release, improved cardiovascular fitness, and reduced inflammation, which are all associated with improved mental health. Physiologically, HIIT enhances cardiorespiratory fitness by improving cardiac output and circulation, positively impacting the nervous system and alleviating anxiety symptoms (57). It increases heart rate variability, which is associated with better autonomic nervous system regulation, thereby contributing to reduced anxiety levels (62). Additionally, high-intensity exercise promotes the release of endorphins, natural pain-relieving substances that enhance mood and decrease feelings of anxiety (63). HIIT may also help regulate cortisol levels, a hormone linked to stress responses, where elevated levels are associated with anxiety symptoms (64). Studies suggest that HIIT can lower inflammatory markers in the body, such as C-reactive protein (CRP), helping to reduce chronic low-grade inflammation, which positively influences anxiety (65). From a psychological perspective, HIIT boosts participants’ sense of self-efficacy by completing challenging tasks, making them more confident and better equipped to handle daily stressors (66). During exercise, attention shifts from anxiety sources to the activity itself, providing temporary relief from anxious feelings (64) and promoting cognitive improvements. Furthermore, the sense of accomplishment and enjoyment derived from HIIT contributes to increased positive emotions and decreased negative emotions, thus alleviating anxiety (67). Long-term engagement in HIIT can enhance coping strategies, enabling individuals to adopt more proactive and effective approaches to managing their anxiety (68).
4.2 Strengths and limitationsThis study employed a scoping review methodology to systematically collect and analyze relevant literature on the impact of HIIT on anxiety, ensuring comprehensiveness and representativeness of the research (69). Rigorous literature screening criteria were applied to ensure the quality of the included studies, enhancing the reliability of the findings (70). This review not only evaluated the direct effects of HIIT on anxiety symptoms but also explored how baseline anxiety levels influenced the effectiveness of the training, providing a multi-dimensional analysis. The use of standardized psychological measurement tools, such as the Beck Anxiety Inventory (BAI) and the State-Trait Anxiety Inventory (STAI), ensured the comparability and scientific rigor of the study results.
Despite including multiple studies, several individual studies had small sample sizes. This issue significantly impacts the generalizability and robustness of the findings, as smaller samples are more susceptible to bias and variability, which can lead to less reliable results (57). Studies with small sample sizes often lack the diversity needed to represent broader populations accurately. Random fluctuations in participant characteristics or responses can disproportionately influence the results, leading to overestimation or underestimation of the actual impact of HIIT on anxiety. The duration of HIIT training in the reviewed studies was relatively short (typically around six weeks), which may not fully capture the long-term impact of HIIT on anxiety (58). Additionally, the HIIT protocols varied across studies in terms of training frequency, intensity, and duration, potentially leading to heterogeneity in the results (71). Additionally, small samples are more prone to selection bias, where the characteristics of participants might not be representative of the target population, further compromising the reliability of the outcomes. When small-sample studies are included in meta-analyses or systematic reviews, the overall conclusions drawn from these analyses can be skewed. Furthermore, the studies did not adequately address the impact of factors such as social support on anxiety symptoms, which may significantly influence the effectiveness of HIIT interventions on mental health (72). While this review examined the influence of baseline anxiety levels, other individual differences—such as genetic background and lifestyle habits—may also affect the efficacy of HIIT (69). Therefore, future research should aim for larger, more diverse samples to enhance the robustness and generalizability of findings.
Furthermore, the potential role of social support in enhancing the effectiveness of HIIT should not be underestimated. Social support, including encouragement from trainers, companionship from fellow participants, and reinforcement from family and friends, can significantly influence adherence to exercise regimens and boost motivation (73). Participants who receive robust social support are more likely to maintain consistent attendance and push through the challenging aspects of HIIT, leading to better psychological outcomes and sustained reductions in anxiety. Moreover, social interactions within group settings can foster a sense of community and belonging, which can directly alleviate feelings of isolation and improve mental health. Conversely, a lack of social support may result in decreased motivation, higher dropout rates, and less favorable outcomes. Therefore, future studies should consider integrating measures of social support into their analyses to fully understand its impact on the effectiveness of HIIT interventions (74).
5 ConclusionsThis scoping review highlights the effectiveness of high-intensity interval training (HIIT) in alleviating anxiety symptoms, particularly among individuals with lower initial levels of anxiety. The clinical utility of HIIT as a therapeutic approach is noteworthy, offering a valuable option for those who favor treatments that do not rely on medication. By personalizing HIIT programs to match individual anxiety levels and considering longer training periods, sustained improvements over time can be achieved. Integrating HIIT with psychological therapies like cognitive behavioral therapy (CBT) and fostering social support significantly enhances outcomes for anxiety management, making it a robust, non-pharmacological tool that appeals to patients seeking alternatives beyond traditional drug-based interventions.
6 Practical recommendationsFuture research should include extended follow-up periods to assess the enduring effects of HIIT on anxiety and focus on large-scale clinical trials using validated methods to better understand its efficacy and dose-response relationship. To maximize benefits, healthcare providers are encouraged to tailor HIIT programs to individual needs, consider longer training durations, and integrate HIIT with psychological therapies such as CBT. Fostering social support and creating environments that encourage adherence to HIIT programs can further enhance treatment outcomes, providing diverse and empowering pathways for individuals to improve their mental well-being.
Author contributionsYW: Conceptualization, Investigation, Writing – original draft. HZ: Methodology, Software, Writing – review & editing. XZ: Data curation, Methodology, Writing – original draft. YZ: Methodology, Software, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported in part by the award to ST from Texas Physical Therapy Foundation.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statementThe author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1515266/full#supplementary-material
References1. Ren L, Fan Y, Wu W, Qian Y, He M, Li X, et al. Anxiety disorders: Treatments, models, and circuitry mechanisms. Eur J Pharmacol. (2024) 983:176994. doi: 10.1016/j.ejphar.2024.176994
PubMed Abstract | Crossref Full Text | Google Scholar
2. Vos T, Abajobir AA, Abbafati C, Abbas KM, Abastabar H, Aboyans V. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2017) 390:1211–59. doi: 10.1016/S0140-6736(17)32154-2
PubMed Abstract | Crossref Full Text | Google Scholar
3. Freud S. Collected papers Vol. 1. Hogarth: London (1924).
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-V. 5th ed. Arlington: American Psychiatric Association (2013).
6. Batelaan NM, Seldenrijk A, Bot M, van Balkom AJLM, Penninx BWJH. Anxiety and new onset of cardiovascular disease: critical review and meta-analysis. Br J Psychiatry. (2016) 208:223–31. doi: 10.1192/bjp.bp.114.156554
PubMed Abstract | Crossref Full Text | Google Scholar
7. Momen N, Plana-Ripoll O, Agerbo E, Benros ME, Børglum AD, Christensen MK, et al. Association between mental disorders and subsequent medical conditions. N Engl J Med. (2020) 382:1721–31. doi: 10.1056/NEJMoa1915784
PubMed Abstract | Crossref Full Text | Google Scholar
8. Iancu SC, Batelaan NM, Zweekhorst MBM, Bunders MBM, Veltman JFG, Penninx DJ, et al. Trajectories of functioning after remission from anxiety disorders: 2-year course and outcome predictors. Psychol Med. (2014) 44:593–605. doi: 10.1017/S0033291713001050
PubMed Abstract | Crossref Full Text | Google Scholar
9. Alonso J, Liu Z, Evans-Lacko S, Sadikova S, Sampson NA, Chatterji, et al. Treatment gap for anxiety disorders is global: results of the World Mental Health Surveys in 21 countries. Depress Anxiety. (2018) 35:195–208. doi: 10.1002/da.2018.35.issue-3
Crossref Full Text | Google Scholar
11. Laursen PB, Jenkins DG. The scientific basis for high-intensity interval training: optimising training programmes and maximising performance in highly trained endurance athletes. Sports Med (Auckland N.Z.). (2002) 32:53–73. doi: 10.2165/00007256-200232010-00003
PubMed Abstract | Crossref Full Text | Google Scholar
13. Morres ID, HatziGeorgiadis A, Stults-Kolehmainen MA, Arpin-Cribbie C, Kavussanu M, Theodorakis Y. Aerobic exercise for adult patients with major depressive disorder in mental health services: A systematic review and meta-analysis. Depression Anxiety. (2018) 35:40–54. doi: 10.1002/da.22842
PubMed Abstract | Crossref Full Text | Google Scholar
14. Coates AM, Joyner MJ, Little JP, Jones AM, Gibala MJ. A perspective on high-intensity interval training for performance and health. Sports Med. (2023) 53:85–96. doi: 10.1007/s40279-023-01938-6
PubMed Abstract | Crossref Full Text | Google Scholar
15. Reljic D, Lampe D, Wolf F, Zopf Y, Herrmann HJ, Fischer J. Prevalence and predictors of dropout from high-intensity interval training in sedentary individuals: A meta-analysis. Scandinavian J Med Sci sports. (2019) 29:1288–304. doi: 10.1111/sms.13452
PubMed Abstract | Crossref Full Text | Google Scholar
16. de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J physiotherapy. (2009) 55:129–33. doi: 10.1016/S0004-9514(09)70043-1
PubMed Abstract | Crossref Full Text | Google Scholar
17. Yan L, Wei JA, Yang F, Wang M, Wang S, Cheng T, et al. Physical exercise prevented stress-induced anxiety via improving brain RNA methylation. Advanced Sci (Weinheim Baden-Wurttemberg Germany). (2022) 9:e2105731. doi: 10.1002/advs.202105731
PubMed Abstract | Crossref Full Text | Google Scholar
18. Wegner M, Helmich I, MaChado S, Nardi AE, Arias-Carrion O, Budde H. Effects of exercise on anxiety and depression disorders: review of meta- analyses and neurobiological mechanisms. CNS neurological Disord Drug Targets. (2014) 13:1002–14. doi: 10.2174/1871527313666140612102841
PubMed Abstract | Crossref Full Text | Google Scholar
19. Urrútia G, Bonfill X. Dealing with bias in systematic reviews of interventions. J Royal Soc Med. (2010) 103(8):364–9. doi: 10.1258/jrsm.2010.100063
Crossref Full Text | Google Scholar
20. Stubbs B, Vancampfort D, Rosenbaum S, Ward PB, Schuch FB, Richards J, et al. How much physical activity do people with schizophrenia engage in? A systematic review, comparative meta-analysis and meta-regression. Schizophr Res. (2017) 186:94–102. doi: 10.1016/j.schres.2016.05.017
PubMed Abstract | Crossref Full Text | Google Scholar
21. Weston M, Taylor KL, Batterham AM, Hopkins WG. Effects of low-volume high-intensity interval training (HIT) on fitness in adults: A meta-analysis of controlled and non-controlled trials. Sports Med. (2014) 44:1005–17. doi: 10.1007/s40279-014-0180-z
PubMed Abstract | Crossref Full Text | Google Scholar
22. Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med Sci Sports Exercise. (2011) 43:1334–59. doi: 10.1249/MSS.0b013e318213fefb
留言 (0)