Study design
The Fre-Phy-Mig study is a single-centre, longitudinal prospective observational study. The study was performed in accordance with the principles of the declaration of Helsinki and was approved by the Valladolid East Clinical Research Ethics Committee PI 21-2408. All participants signed an informed consent form to participate in the study. The study was reported following the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement [15].
Setting
The study was conducted in the headache outpatient clinic of the Hospital Clinico Universitario de Valladolid, Spain, a third-level, university, public hospital. Concerning the study period, data collection spanned from 30 July 2021 (first patient- first visit) to 03 July 2023 (last patient - last visit). All participants were followed for three months.
Participants
The study population was composed of patients who started preventive treatment with fremanezumab (monthly), according to the criteria of the responsible physician and the local standard of care and clinical practice guidelines [16]. In the Spanish public healthcare system, CGRP monoclonal antibodies were subsidized in chronic migraine patients if they had previously failed to at least three migraine preventives, including onabotulinumtoxinA [16, 17]. Participants were included in the study if: (1) were aged between 18 and 65 years; (2) fulfilled criteria for chronic migraine (with or without aura) according to the International Classification of Headache Disorders (ICHD, 3rd version) [6]; (3) reported a migraine onset at least one year prior to the study onset; (4) were able to complete questionnaires. Patients were excluded if they: (1) had previously received another drug against CGRP; (2) presented other primary or secondary headache disorders, except for low-frequency tension-type headache or medication overuse headache; (3) had unusual migraine subtypes such as hemiplegic migraine (sporadic and familial), ophthalmoplegic migraine, migraine with neurological symptoms that are not typical of migraine aura (diplopia, altered consciousness or long duration); (4) had any clinically relevant cognitive or psychiatric disorder; (5) exhibited any pathology that could be a contraindication to physical exercise according to the guidelines of the Spanish Society of Sports Medicine (SEMED-FEMEDE) [18]; (6) were pregnant, expressed gestational desire, or breastfeeding; (7) were illiterate or had insufficient Spanish language performance.
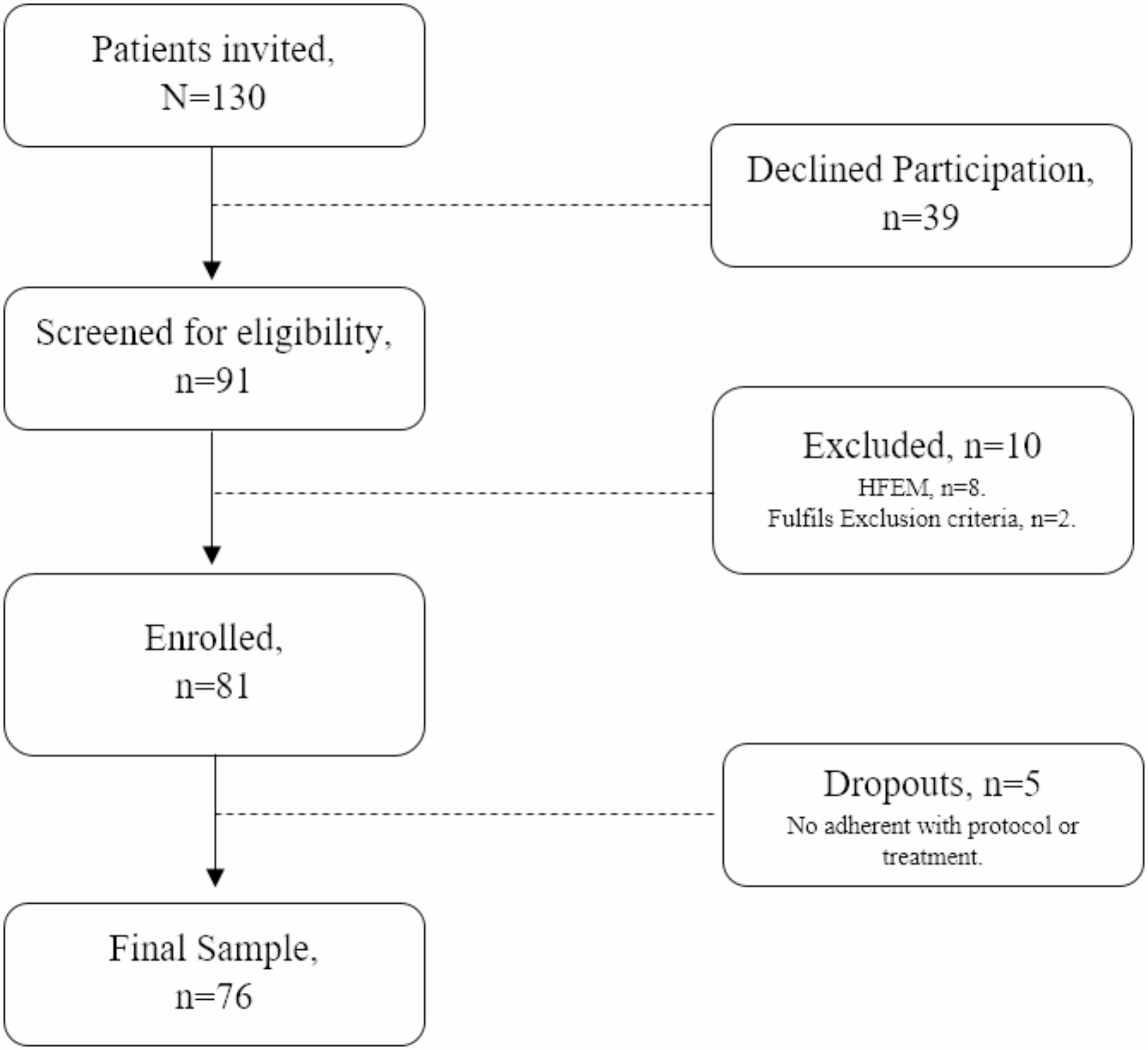
Recruitment was done in the headache unit, where all consecutive patients were screened for eligibility and were invited to participate. Follow-up was conducted by in-person and telephone visits by healthcare providers.
Variables
A structured clinical interview was performed by a trained-physician. Demographic and anthropometric variables included sex, age, and educational level, weight, height and body mass index (BMI). Prior and current history of psychiatric disorders and fibromyalgia was assessed. Clinical variables included the specific migraine diagnosis, according to the ICHD-3 (with/without aura; chronic migraine), age of onset, months of evolution of chronic migraine, the prior number of migraine preventive drugs classes, and the presence of medication overuse headache (MOH). Furthermore, headache days per month (HDM), migraine days per month (MDM), non-steroidal anti-inflammatory drugs (NSAIDs) and acetaminophen days per month (ADM), triptan days per month (TDM), and the median intensity of headache (MIH) episodes was measured in a 0–10 numeric verbal analogue scale (VAS) [19]. The adverse headache impact was assessed by the Headache Impact Test – 6 (HIT-6) [20]. Finally, physical activity and time sitting levels were evaluated using The International Physical Activity Questionnaire long-form (IPAQ-LF).
Physical activity / exposure variable
The IPAQ-LF was adopted to collect data on Physical Activity (PA) and Time Sitting levels (TS) [21]. The tool quantifies physical activity in adults and can be used by either by telephone or self-administered [22]. The questionnaire has been previously translated and validated in the Spanish population [23]. The IPAQ collects data regarding the PA levels over the prior seven days. The information can be divided across five domains, including work, household, leisure-time, commuting, and time sitting. Each domain can be subdivided by the intensity of the activity thus we can distinguish between walking, moderate and vigorous. Information of each domain is collected using questions such as: “during the last 7 days, on how many days did you walk for at least 10 minutes at a time in your leisure-time?” and “How much time did you usually spend on one of those days walking in your leisure-time?”. IPAQ-LF requires between 15 and 30 min to be administered [22].
PA and TS levels were extracted and analysed following international guidelines [22]. Sum total of all domains (IPAQ-All domains) was obtained of the sum of all time invested by the participant in each domain (minutes/week). Leisure-time physical activity was obtained from the global computation of the sum of the three intensities of that domain (walking, moderate intensity, vigorous intensity) in minutes/week. Time spent walking was obtained from the global computation of the sum of the two domains: transportation and leisure-time (minutes/week). Time spent sitting (TS) was obtained from the average number of hours/day spent in a sitting or lying position. Total metabolic equivalent (METs) was calculated so that walking-intensity, moderate-intensity and vigorous-intensity accounted for 3.3, 4.0 and 8.0 METs, respectively. Thus, walking, moderate and vigorous MET-min/week were calculated by multiplying the selected MET value by the minutes/week of each intensity. The total PA MET-min/week was obtained by summing up the walking, moderate and vigorous MET-min/week score. A category analysis according to Data processing guidelines of the IPAQ-LF was considered, distinguishing category levels: low, moderate and high [24].
Finally, as workloads throughout the protocol changed and may be a confounding factor, work-domain physical activity and time sitting during week-days were dropped from the analysis. Moreover, calculations of bicycle use in transportation were not included, because no participants used this transport method through the study period. Only physical activities performed for at least 10 min per week were computed. The questionnaire was used in the hetero-administered form.
Data sources /measurement
Data sources were clinical or telephone interview, using electronic and paper medical records. The survey data was collected on a standardized pre-defined template in paper format. The patients were diagnosed by headache neurologists. As per local standard of care and requirement for receiving CGRP mAb within the national healthcare system, all patients prospectively completed a headache diary, which included HDM, MDM, ADM, TDM, MIH. Intensity of headache episodes was evaluated according to VAS intensity rating scale, which consists in a 100-mm line with the end points of 0 (no pain) and 10 (worst pain) [19]. Response to fremanezumab was evaluated between weeks 8–12, compared with the month prior to the treatment use, as a reduction of ≥ 50% in the number of migraine days [25]. Furthermore, partial response was defined as a reduction of ≥ 30% in the number of migraine days between weeks 8–12 compared to baseline; and super-response was defined as a reduction of ≥ 75% in the number of migraine days between weeks 8–12 compared to baseline. The negative impact of headache was assessed by the Headache Impact Test – 6 (HIT-6), which includes six questions that are scored between 6 and 13, with a final score between 36 and 78. The score is stratified into four categories: little or no impact (< 50), some impact (50–55), substantial impact (56–59) and severe impact (> 59) [20].
Intervention
The study period was divided in three prospective visits (further information is specified in the Supplementary Material): During baseline visit (T0), prior to any study procedures patients were informed about the study and were requested to provide consent to participate, clinical data was obtained from the headache calendars, and IPAQ-LF was administered. This T0 visit prior to the beginning of fremanezumab treatment.
The second and third visit took place one and three months after the fremanezumab administration (T1m and T3m, respectively). During these visits, clinical data was retrieved from headache calendars and the IPAQ-LF was administered.
Bias
A series of biases were anticipated in the study design. Details are available in the Supplementary Material.
Statistical methods and sample size
Descriptive statistics were used to examine the sociodemographic and clinical characteristics of the sample. Normal distribution of variables was tested by the Kolmogorov Smirnov test. Continuous quantitative variables were described as mean and standard deviation or median and interquartile range, depending on the type of distribution. Continuous variables in related groups were analysed using Wilcoxon test. For the correlations analysis between PA and clinical variables, the bilateral Spearman’s Rho test was used (Rs).
To assess the primary outcome and evaluate whether the levels of PA at baseline were associated with a different probability of response, a logistic regression analysis was done. The dependent variable was a 50% responder rate. First, a univariable regression analysis was conducted, and all the variables that showed a P value < 0.2 were included in a multivariable analysis. Odds ratios (OR) and their 95% confidence intervals (CI) are described. Due to the exploratory nature of the study, the substantial number of variables and the insufficient evidence to select the variables based solely on the literature, a stepwise multivariable regression analysis was done, employing the backwards procedure and the Wald method. We adjusted for multiple comparisons by using the False Discovery Rate (FDR) with Benjamini-Hochberg procedure [26]. In order to facilitate the data interpretation in the multivariate test, variables using minutes/week or minutes/day were converted to hours/week or hours/day. In all hypothesis tests performed, p-value < 0.05 was considered statistically significant.
Sample size calculation was based in another national study based on the same preventive-guidelines included 129 patients per year [17, 27]. Previous 21.3% increase in walking levels previously reported in a manuscript with equivalent population [28] was considered. Using a precision of 5.9% and a CI of 95% we obtained a final sample size of 76 patients. Concerning missing data, imputation methods by linear regression was used (clinical variables and physical activity variables at baseline and after three months had no missing data). The study analysis was performed as per protocol. For data analysis, the Statistical Package for Social Sciences (SPSS®, version 27.0, IBM Corp. Armonk, N.Y.) was used.


留言 (0)