Tuba Cerrahoğlu Şirin, Arife Gonca KapıcıoğluUniversity of Health Sciences, Şişli Hamidiye Etfal Training and Research Hospital, Neurology Department, İstanbul, Türkiye
The Journal of Headache and Pain 2024, 26(Suppl 1):O5
Background
Chronic migraine (CM) is defined as headaches occurring for at least 3 months, with ≥15 headache days per month, of which 8 or more are migraine attacks. Many patients first seek neurological care when their migraine has progressed to the CM stage, often complicated by medication overuse headache (MOH), making management challenging. While topiramate (TPM) and OnabotulinumtoxinA (OBontA) are proven to be effective in CM, TPM's side effects and OBontA's high cost necessitate exploring alternative treatment approaches in some cases.
Objective
This study aimed to investigate effective treatment approaches in the management of chronic migraine, particularly in cases with concomitant MOH.
Methods
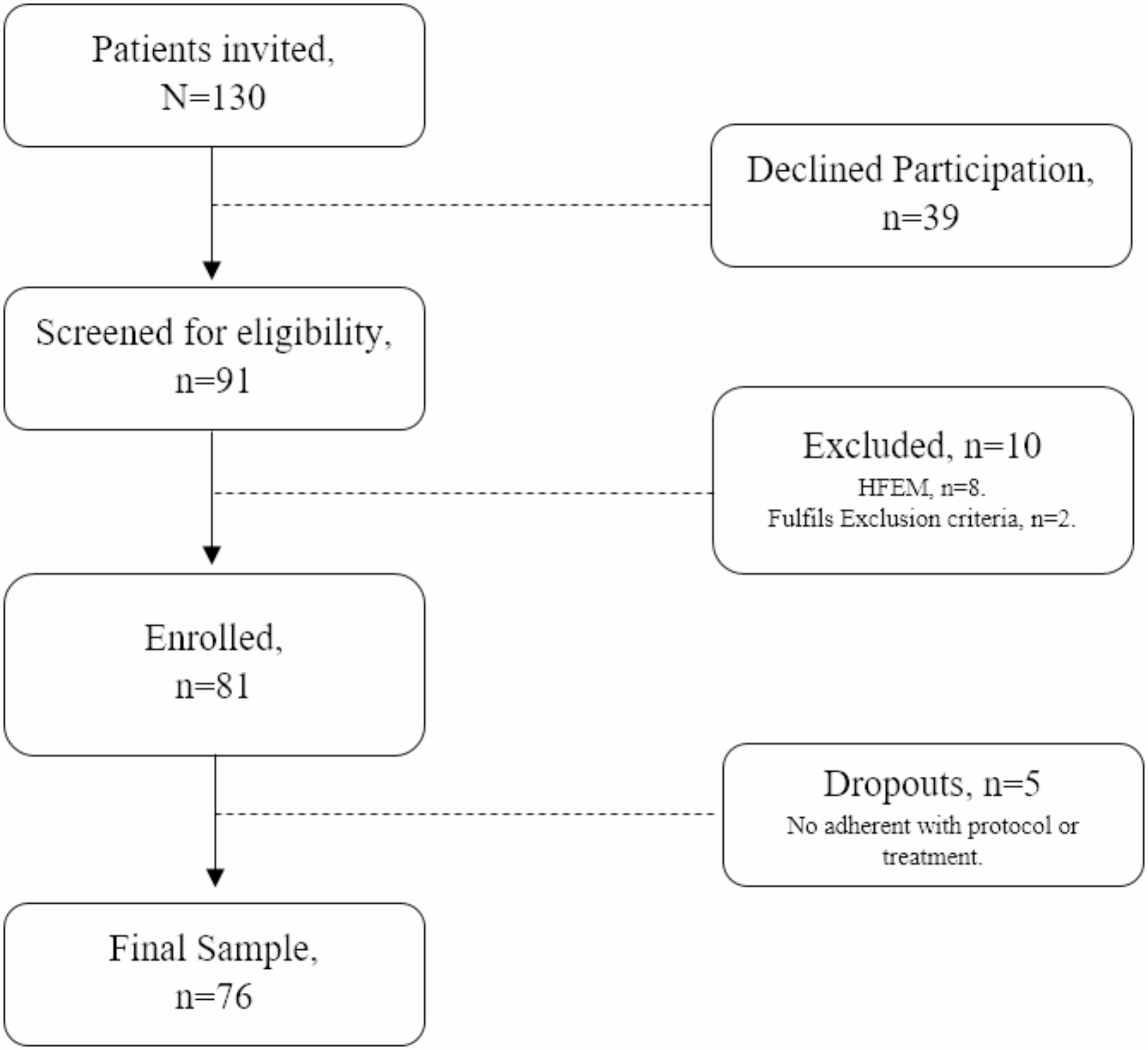
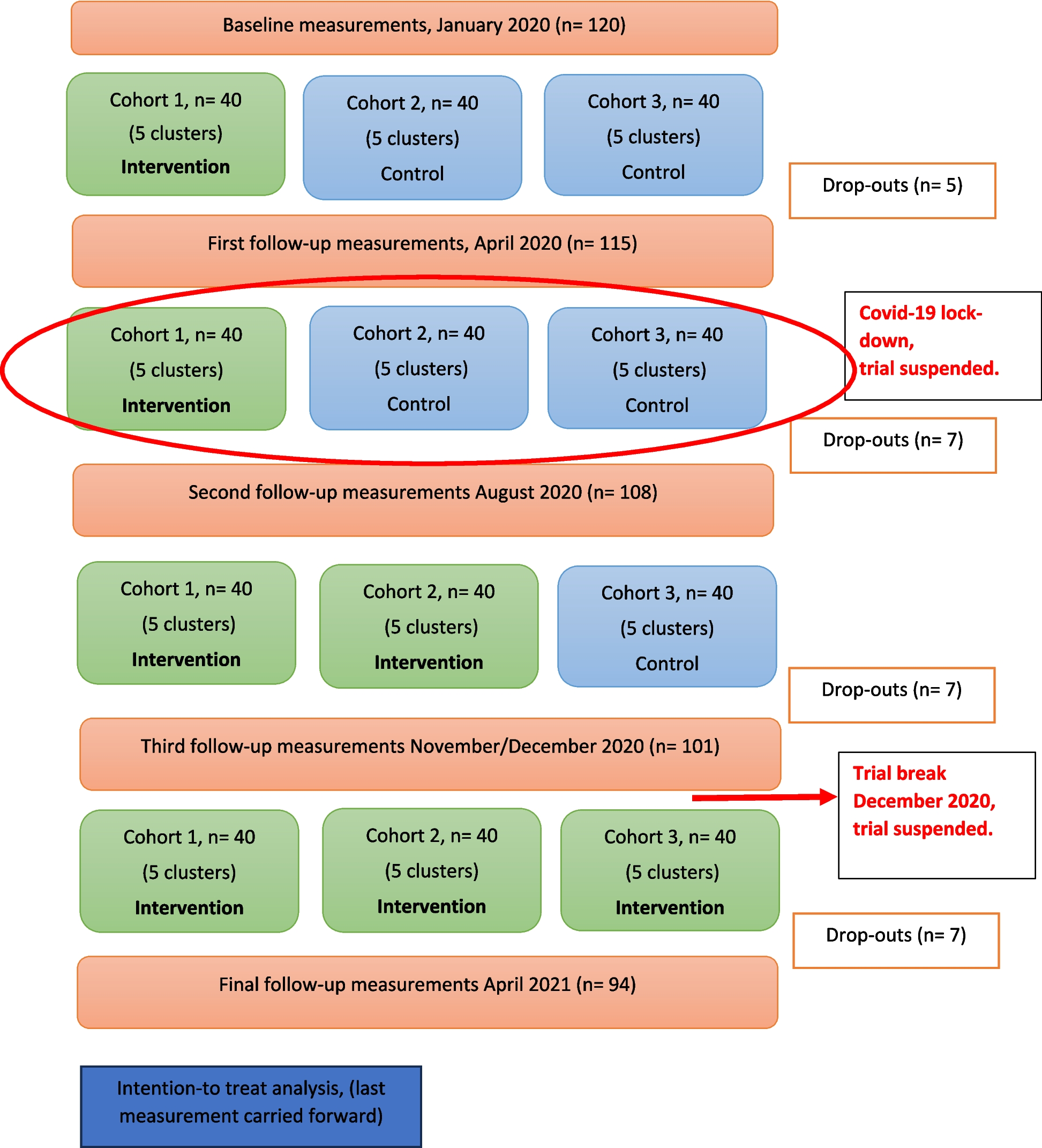
A retrospective review was conducted of patients diagnosed with CM who were followed at the Headache Clinic between January 2023 and September 2024. Data collected included patients' migraine history, presence of MOH, treatments administered during follow-up, and whether patients transformed from CM to episodic migraine (EM). Attack frequency was classified as low-frequency EM (LFEM, <7 days/month) or high-frequency EM (HFEM, ≥7 days/month).
Results
The study included 43 patients with CM, with a mean age of 40 years. The majority (93%) were female, and the mean disease duration was 16 years (range: 2–37 years). Concomitant MOH was present in 72% of patients, and 55% had a history of failed prophylactic treatment despite appropriate dosage and duration. After treatment, 58% of patients transformed to LFEM and 37% to HFEM. CM persisted in only 2 patients (4.6%) despite combined treatments, including oral prophylaxis, CGRP monoclonal antibodies (CGRPmAb), and OBontA.
The most effective treatment combinations for transforming CM into LFEM were peroral prophylaxis (PO) plus nerve block (48%), nerve block alone (16%), OBontA + PO + nerve block (12%), OBontA alone (8%), PO alone (8%), OBontA + nerve block (4%), and PO + transcranial direct current stimulation (tDCS) (4%). For transforming CM into HFEM, the most effective treatments were PO + nerve block (56%), nerve block alone (18%), CGRPmAb (6%), CGRPmAb + OBontA (6%), and nerve block + tDCS (6%). There were no significant differences in the presence of MOH (72% vs 68%, p>0.05) or the use of combination therapy between the LFEM and HFEM groups (68% vs 75%, p>0.05). However, the HFEM group had a significantly higher rate of failed prophylaxis compared to the LFEM group (75% vs 40%, p=0.02).
Conclusion
Combination treatment strategies were the most effective in transforming CM to both LFEM and HFEM. Nerve blocks, often added to peroral prophylaxis, provided sufficient efficacy and were preferred due to the high cost of OBontA and CGRPmAb. Although OBontA, CGRPmAb, and tDCS demonstrated good efficacy in combination treatments, nerve blocks should be considered as an earlier, cost-effective intervention before resorting to more expensive options.
Keywords
Chronic migraine, high-frequency episodic migraine, low-frequency episodic migraine, treatment, nerve block, prophylaxis


留言 (0)