Adolescent suicide is a significant mental health issue that affects the public. Adolescents are vulnerable to mental health issues. In children, suicide is comparatively rare, but as adolescents approach puberty, it becomes more prevalent. It ranks among the world's top causes of death for underage individuals. Every suicide is the consequence of a complicated, dynamic, and one-of-a-kind interplay across several important influencing elements, but individual attempts to anticipate and avoid suicide are doomed to failure [18].
Debate still rages about the significance of suicidal risk, especially in adolescence, and its connection to mental illness and committed suicide. Based on several recent research, teenagers' suicide risk was predictive of and linked to psychopathology, including mood, anxiety, and drug use disorders in both adult and adolescent populations. Moreover, it has been connected to emotional and behavioral functioning deficiencies [19]. Therefore, the purpose of the research was to ascertain the prevalence of suicidal ideation and behavior in high school students, comprehend certain predictive factors that aid in the explanation of suicidal ideation between school adolescents in the underdeveloped nations, and identify the risk factors linked to high suicidal scores across various secondary school grades.
553 scholars from public and private schools in Cairo, Egypt, who were enrolled in the tenth, eleventh, and twelfth grades for the academic year 2021–2022 participated in this cross-sectional study. Their ages ranged from 15.25 ± 1.75 on average. 39.7% of those who participated were males, while 60.3% of the respondents were females. Among the students who took part, 27.7% had a history of suicidal ideation, and 13 (2.4%) had a history of suicide attempts. Of the students, 100 (18.1%) engaged in non-suicidal self-injury (NSSI). 0.7% of those participated had a family history of attempts at suicide, whereas 13.7% had a family history of mental illness.
Based on the Suicide Probability Scale, 88.97% of the students who took part were subclinical, and 11.03% had a plausible risk of suicide, with non-significant difference between males and females in all study groups. These findings showed a smaller incidence of suicide than the 24% recorded in 481 students from Santa Marta, Colombia, as determined by the Plutchik suicide risk scale [20]. This was also not the case with the observed rate of 30.5% lifetime suicidal ideation in 2,817 scholars from different government schools in Bogota´ [21] or the 13.7% at some point in life identified in 3,328 scholars from Hong Kong [5] who were using the suicidal behavior measure. Moreover, according to 342 Jamaican students who completed the YOUTH survey, the likelihood of suicidal ideation was less than 38% of all times [22]. The various time periods examined, the various measures employed in each study, the standards for measuring teenage suicidal ideation, and the variations in the sociocultural traits of the students who took part in every investigation could all contribute to the fluctuations in incidence [3, 23].
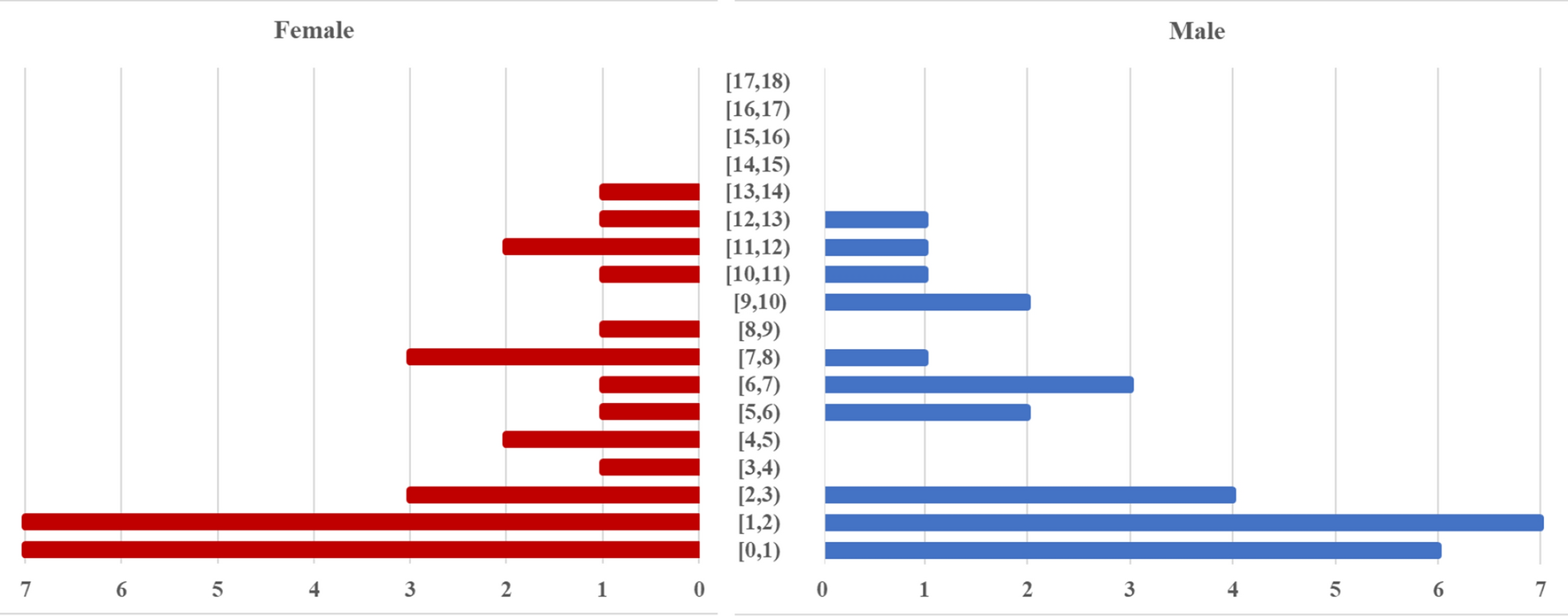
The adolescents in the current study ranged in age from 13 to 17 years, with a mean (± SD) age of 15,25 ± 1.75 years. The group of third-year students, aged 17.3 ± 0.24, had more suicidal ideation, whereas the group of second-year students, aged 16.2 ± 1.2, had higher suicidal attempts. Third-year students had the largest percentage of severe cases (2.8%), whereas second-year students had the highest percentage of subclinical cases (91.5%). These findings corroborated the findings of Stephanie and colleagues [24], who stated that throughout 2006 and 2015, 273 successful suicides involving people aged 10 to 19 were recorded: none involving those aged 10 to 12. The incidence of teenage suicide increases significantly with age, as seen by the 171 (63%) suicides that occurred in the older adolescent group (17–19 years) and the 102 (37%) suicides that occurred in the younger adolescent group (13–16 years). This maturing takes place as teenagers are going through biological and psychological transformations related to growing up, as well as sociocultural shifts brought on by the transition from childhood to maturity.
Regarding the higher risk of suicide within females than males, this study noted that females had suicidal attempts more frequently (12.9%) than males (8.2%). These findings are consistent with the 2017 statistics from the Youth Risk Behaviour Surveillance System (YRBSS), which offers insightful information about adolescent suicide trends. The data also demonstrate that, overall, the proportion of high school students who indicate seriously thinking about suicide has increased since 2009, with female students experiencing the largest growth in this regard. Male rates were 10.3 percent in 2009, while rates were 11.9 percent in 2017 that did not vary appreciably [8].
There was a notable disparity in the incidence rates between the gender-specific reports from the CDC and the present study. The CDC reports that in 2017, women were approximately twice as likely as men to convey seriously thinking about suicide (22 and 12 percent, accordingly), trying suicide (9 and 5 percent, subsequently), and needing medical care (3.1 and 1.5 percent, consequently). Males died by suicide more often than females, even though men are significantly more likely to accomplish in suicide attempts. The gender gap in suicide is another term for this disparity. Since in 2008 and 2015, there were around 1.8 times as many suicide deaths worldwide across men as within women. For instance, in Western nations, men commit suicide three to four times as frequently as women. Specialists have partially attributed this discrepancy in the number of suicide deaths and attempted suicides across the sexes to men employing more lethal methods to end their life. However, there could be additional factors, such as differences in the intensity or novelty of suicide ideation [3].
In comparison to harmonious family environments, quarrelsome home environments in the first, second, and third grades were more common in the mild, moderate, and severe categories of suicide likelihood. Thus, there was a correlation between a high likelihood of suicide ideation and severe familial dysfunction. According to Colombian investigations, dysfunctional family relationships was linked to suicide ideation in Bogota´ scholars (OR = 15.0, 95% CI 8.4–26.9), which is in line with earlier findings that was done by Gonza and colleagues [21]. In addition to hindering emotional development, trust, and connection among family members, dysfunctional, acrimonious, and unstable familial relationships have been shown to be predictive of teenage suicidal ideation [25].
Furthermore, the study's findings in the same line with the findings of Lin and colleagues [26]. They reported that adolescents in dysfunctional households had a 3.7-fold higher risk of suicidal ideation than children in harmonious families." Thus, it is imperative to emphasize the significance for familial harmony as a preventive and prediction contributor to teenage suicidal ideation [3]. According to this viewpoint, among the most significant environments for the development of connections that are built on the cooperation, support, and backing of its members is the home [27]. The proper role of the family fosters adaptive strategies for managing psychological discomfort and managing impulses, which in turn promotes mental health and lowers suicidal thoughts and actions. Additionally, the strongest defense against unfavorable circumstances, including sexual misconduct, which can trigger suicidal ideation and attempts, is an effective family role [28].
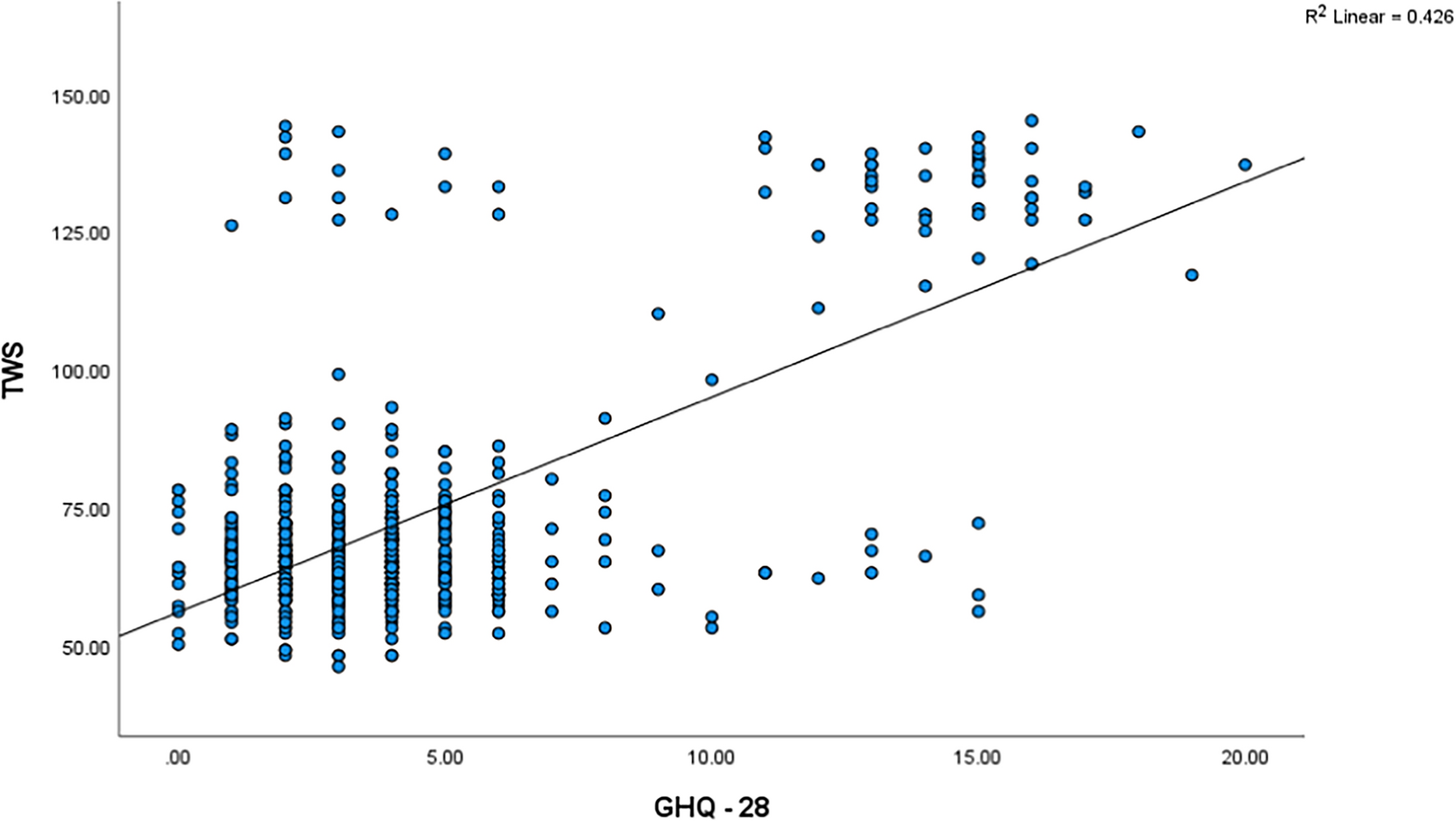
The current finding for the suicidal behavior among teenage in school different school years, were in line with Bauer and colleagues [29], who identified prior mental health conditions as an important risk component and concluded that "Most investigations concur that suicide is tightly associated with psychiatric disorders", the research found that the likelihood of psychiatric disease was 21.8%, 16.1%, and 15% in the first, second, and third years, respectively. Additionally, there was a substantial positive association among the suicide likelihood score and the total GHQ-28 score. Ninety percent of the subjects who take their own lives have at least one mental illness. It has been discovered that among 47 and 74% of the risk of suicide is associated with psychiatric conditions. The most prevalent disorder in these situations is emotional disturbance. It was discovered that personality disorders like borderline or antisocial disorders of personality were present in 30–40% of the participants who conducted suicide. In the same meaning, Bilsen [12] discovered that, whereas schizophrenia alone accounts for a very small percentage of all youth suicides, suicide is frequently the primary cause of death for adolescents with eating problems, particularly anorexia nervosa.
The results of the current study were in the opposite with the findings of Bilsen [12], who reported that approximately 25–33% of all suicide cases were started by a previous suicide try, an issue that was more common among males than females where the current study showed the issue were higher in females than males. Besides, the study also revealed that non-suicidal self-injury (NSSI), previous experience of suicidal ideation, and the existence of past suicide attempts had a substantial connection with higher suicidal scores among first-, second-, and third-year students. According to research, boys who have made previous tries at suicide are 30 times more likely to try suicide than boys who have not. The risk of suicide is tripled for girls who have attempted suicide in the past. Research indicates that 1–6 percent of individuals who try suicide pass away within the first year. It has been discovered that the self-inflicting act itself carries a greater risk of suicide than the level of suicidal purpose involved in the act [12].
Furthermore, the current study reported that groups with moderate and severe suicide probability were linked to less than adequate financial status. These findings were consistent with the findings of a large systemic review investigation by Bantjes and colleagues [30] who determined that 75 percent of suicides takes place in countries with middle and low incomes (LMICs), in which rates of impoverishment are high. Research points to a connection between suicidal ideation and financial variables [30].
The present study highlights the issue suicide among Egyptian adolescence as one of poorly investigated topics in middle- and low-income countries. The substantial suicide death rate among young people in low- and middle-income nations is a cause for worry. One of the sustainability goals for non-communicable illnesses that the WHO outlines in its Global Action Strategy is to cut the suicide rate by one-third among 2015 and 2030 [31]. If the present patterns keep going, only 3% of 118 nations will meet this goal despite the limited data available, underscoring the necessity for governments worldwide to enhance their suicide data and implement multimodal preventive measures to drastically lower suicide rates [32].
Some limitations were identified, the study relied on students' self-reported impressions determined by their personal evaluations of their risk for suicide, which may have resulted in recall bias or incompletely realistic responses. Furthermore, the cross-sectional study's design precluded any information regarding causality. It is recommended to involve larger sample size, multi-centric layout, long-term research in the future to assess the link among Egyptian adolescent’s suicide risk and stress and mental health disorders. It also recommended to start an effective program by practitioners, program developers, and researchers to avoid this issue as recommended by other investigators [33, 34].




留言 (0)