SBD is a heterogeneous group of monogenic diseases characterized by increased bone density. This group includes 40 disease entities, such as osteopetrosis, dysosteosclerosis, sclerosteosis, and CTDI [7]. Many of SBD patients suffer from visual loss due to compression of optic nerve at the optic canal in the base of the skull caused by osteosclerosis as seen in the patient reported here [1,2,3].
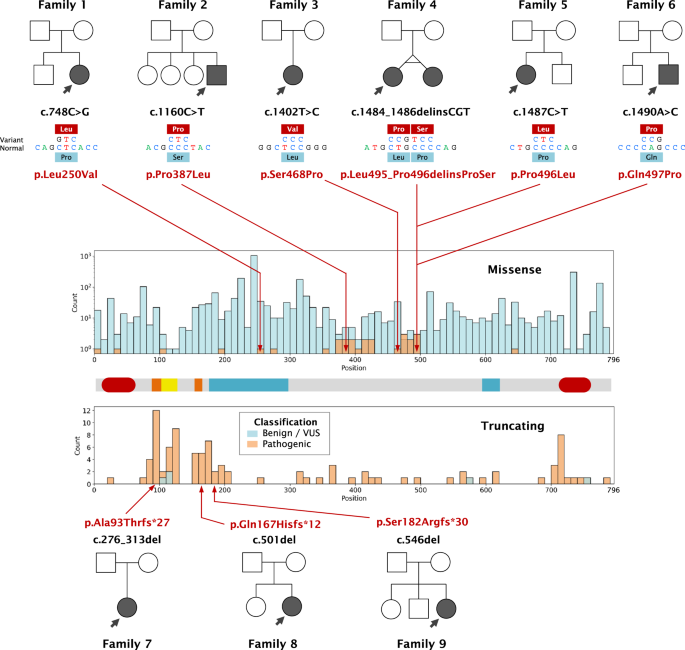
CTDI is caused by bi-allelic pathogenic variants in the TMEM53 gene. This gene encodes for a protein, TMEM53, a transmembrane protein that spans the outer layer of the nuclear envelope of osteoprogenitor cells. Normally, TMEM53 inhibits the BMP-SMAD signaling pathway, which is crucial for bone formation. When TMEM53 is defective, the inhibition of this pathway is lost, leading to accelerated osteogenesis in affected individuals [1,2,3, 8]. Six pathogenic variants have been previously found, most of which are null pathogenic variants; only two heterozygous missense pathogenic variants has been identified in compound heterozygous patients [2, 3]. This is the first report of the patient with biallelic missense pathogenic variants (Supplemental Table 2).
Skeletal disorders of CTDI are not so severe as a skeletal dysplasia. Prognosis of CTDI is determined by visual loss; CTDI patients often experience visual loss during early childhood due to optic nerve compression in the base of the skull. Guo et al. reported a proband who received decompression of optic nerves at age 10, which was not successful [1]. Whyte et al. reported a 10-year-old boy who had bilateral progressive loss of vision and hearing. Treatment with prednisone, optic canal decompression, optic nerve sheath fenestration, and zoledronate were all ineffective [2]. Ommeren et al. showed a 13-year-old boy with CTDI and keratoconus who later developed optic canal narrowing, which caused significant visual loss in one eye. This patient underwent surgical decompression, leading to improved vision acuity and the resolution of papillary edema [3].
Compared with the previous cases, the treatment of our case was successful. After optic canal decompression, the patient was visually functional; he walked without assistance and performed all home tasks by himself. We attribute this success to several factors. First, appropriate early decision-making was based on a series of in-depth ophthalmological evaluations. By closely monitoring the patient’s visual function and the progression of optic canal narrowing through regular ophthalmological examinations, we were able to determine the optimal time for intervention. Second, the skills of our experienced orbital surgeon played a significant role. The surgeon’s proficiency in handling complex optic canal surgeries ensured the safety and effectiveness of the procedure. The meticulous surgical technique and decompression process minimized damage to surrounding tissues.
Compared to other SBD, compression of the optic canal in CTDI progresses slowly. Therefore, loss of vision can be prevented through early recognition and intervention. We recommend early ophthalmology work up and timely intervention by expert surgeons.
Web resources
1000 Genomes, http://www.internationalgenome.org/
dbSNP, https://www.ncbi.nlm.nih.gov/projects/SNP/
GenBank, https://www.ncbi.nlm.nih.gov/genbank/
gnomAD Browser, https://gnomad.broadinstitute.org/
Human Gene Mutation Database (HGMD), https://portal.biobase-international.com/hgmd/pro/start.php
Human Splicing Finder, http://www.umd.be/HSF3/
OMIM, http://www.omim.org/
ClinVar, https://www.ncbi.nlm.nih.gov/clinvar/
UniPort, https://www.uniprot.org/
PREDICTSNP webserver, https://loschmidt.chemi.muni.cz/predictsnp1/
DynaMu, http://biosig.unimelb.edu.au/dynamut/
CADD, https://cadd.gs.washington.edu/
Mutation Taster, https://www.mutationtaster.org/
AlphaMissense, https://alphamissense.hegelab.org/
MutPred2, http://mutpred2.mutdb.org/


留言 (0)