In general, the treatment goal for an AIS is to restore blood supply to the afflicted brain region as soon as possible, i.e., within the first few hours following the onset of stroke symptoms.
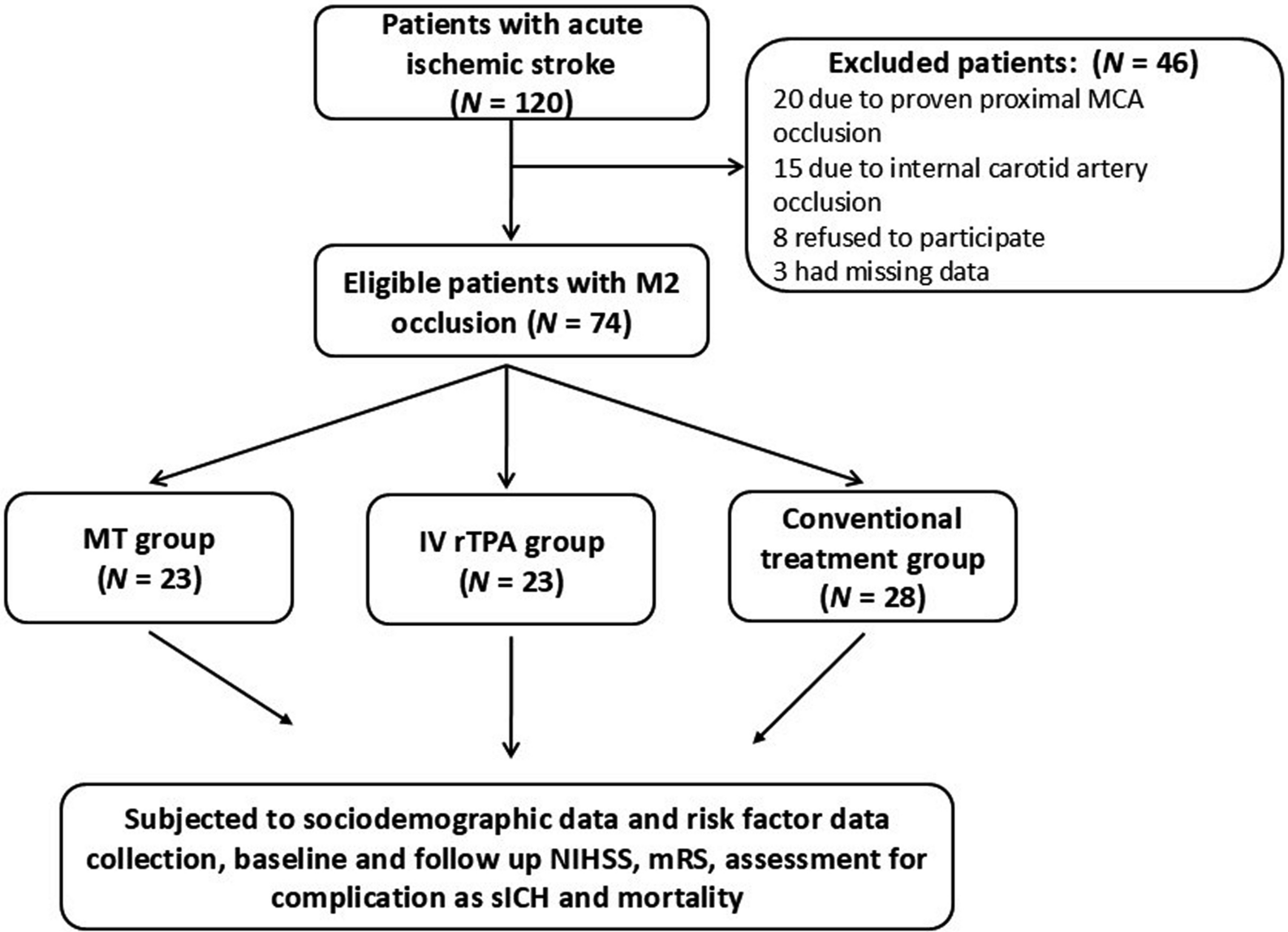
This prospective longitudinal study aimed to compare the outcomes, effectiveness, and safety of MT, IV rTPA, and CMT for treating M2 MCA occlusions as a selective group of AIS in which the MT was scarce. Our analysis of the three groups suggested several potential trends: (1) patients treated with MT and IV rTPA appeared to have better 24-h NIHSS scores compared to those receiving CMT; (2) MT and IV rTPA groups showed a tendency towards improved 3-month mRS scores (≤ 2) relative to the CMT group; (3) successful recanalization after MT (73.9%) was associated with numerically, though not statistically significant, better NIHSS and mRS outcomes; (4) the observed safety profiles, including rates of sICH and mortality were comparable across the three treatment modalities.
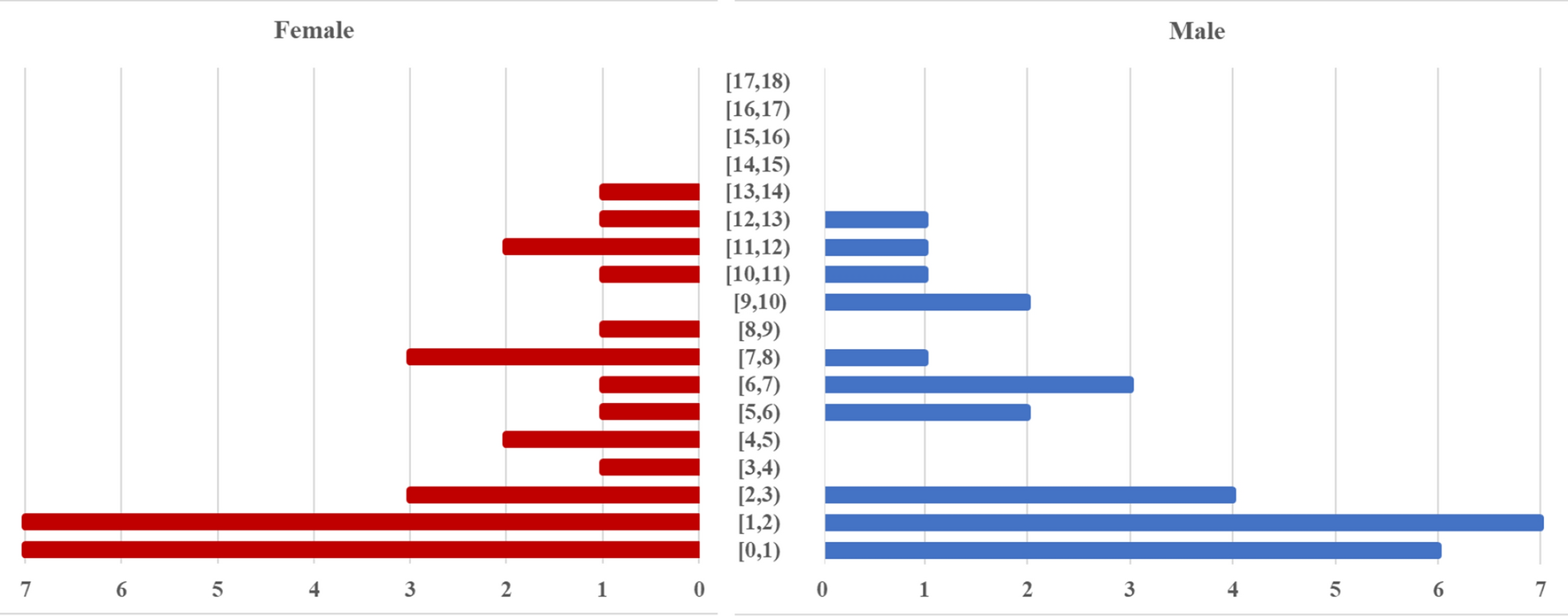
In the current study, the baseline characteristics of the MT group were comparable to the other treatment groups (IV rTPA and CMT) in terms of age and sex distribution. However, the MT group had a higher frequency of DM and hyperlipidemia, while the CMT group had a higher frequency of AF. These observations highlight the importance of optimal management of stroke risk factors and suggest that MT could be advantageous for individuals ineligible for rTPA due to certain risk factors. The increased frequency of AF in the CMT group is likely because many were on anticoagulant therapy, making them ineligible for rTPA. The MT group had a higher NIHSS at admission than the rTPA group, which is similar to the findings of Miura and colleagues [26], who reported that the MT group had a higher baseline score than the rTPA group. Thus, MT may be a second-line treatment for AIS, offering revascularization to high-NIHSS patients ineligible for IV rTPA.
In this study, we did not measure admission glucose levels. However, the high incidence of diabetes, hypertension, and hyperlipidemia among the studied groups may partially explain the poor outcomes. This finding is supported by Bruno and colleagues who found that higher admission blood glucose levels were associated with worse outcomes at 3 months, according to multivariate logistic regression analysis adjusted for stroke severity, diabetes mellitus, and other vascular risks [27].
In the present study, despite MT's higher baseline NIHSS, the MT and IV rTPA groups showed significantly greater improvements in NIHSS scores 24 h following therapy than the CMT group. Also, the MT (69.6%) and IV rTPA (65.2%) groups had better functional outcomes (mRS 0–2) at 3 months compared to the CMT group (7.1%). These findings suggest that MT and IV rTPA interventions may be equally efficacious treatments for M2 occlusions, achieving comparable neurological outcomes in terms of 24-h NIHSS or 3-month mRS scores. These results corroborate previous research indicating potential long-term advantages of MT for M2 occlusion patients [26, 28,29,30,31,32].
Marchal and colleagues found that MT improved neurological and functional results for distal M2 occlusions compared to medical management [29]. A recent meta-analysis by Barchetti and colleagues revealed an overall good functional outcome rate of 58.8% at the 3-month follow-up for MT in distal locations [33]. Vidale and colleagues (2021) conducted a systematic review and meta-analysis, comparing the risk–benefit profiles of MT with or without IV rTPA versus IV rTPA alone in adults with AIS and M2 occlusion. They found similar rates of good functional outcome (mRS < 3) at 90 days between the two strategies, MT versus IV rTPA (62.4% versus 66.3%, respectively) [32]. Moreover, Waqas and colleagues (2021), in their meta-analysis of patients who underwent MT for distal circulation strokes, found that 54.7% of patients who had MT achieved a favorable outcome at 3 months, which was comparable to the 54.5% of IV rTPA [34]. Furthermore, Guo and colleagues (2023) demonstrated in their meta-analysis that MT was associated with better functional outcomes (mRS 0–2) than best medical management in patients with M2 occlusion and moderate-to-severe stroke [28].
The current result suggests the potential benefits of MT in improving functional outcomes and reducing long-term disability in patients with DMVOs, which are often associated with poor prognosis when treated with CMT alone. These findings align with those of Menon and colleagues who reported improved functional independence in patients with M2 segment occlusion who received MT at 90 days compared to those who received the best medical treatment [30]. Similar effects were reported by Sarraj and colleagues (2016) and Miura and colleagues (2019), underscoring the superiority of MT management for M2 occlusions [26, 31].
sICH is the most feared complication of MT [35], especially in smaller vessels which are more vulnerable when treated endovascularly. Saber and colleagues (2018) conducted a meta-analysis of 1080 patients who underwent M2 thrombectomy, comparing them to those with M1 occlusions. The analysis suggests that M2 thrombectomy may carry an increased risk of sICH risk [36]. In the current study, the sICH rates across the three treatment groups appeared to show no notable differences. This observation is consistent with findings from previous studies [29,30,31, 37]. Menon and colleagues found no sICH in patients treated with MT for M2 occlusions compared with a 7.9% rate in the best medical management group (IV-tPA) [30]. Marchal and colleagues reported that sICH occurred in 3.1% of the MT group and 9.5% of the non-MT group [29]. Conversely, Vidale and colleagues found a higher sICH rate in the MT group (8.5%) compared to the IVT group (3%) [32]. Waqas and colleagues reported that 5.8% of patients who underwent MT for strokes in the distal locations experienced sICHs, comparable to 2.5% of patients treated with IV tPA [34].
In the present study, the mortality rate in the MT group appeared to be comparable with that of the other treatment groups, supporting the safety of this treatment modality, as shown in previous studies [26, 28, 37]. Miura and colleagues reported that MT was associated with lower mortality than medical management in a real-world cohort of patients with M2 occlusions [26]. However, Waqas and colleagues reported a 16.5% mortality rate for MT, comparable to 12.4% for IV tPA in treating strokes in distal locations [34]. It is important to consider the potential for susceptibility bias, as patients selected for MT were likely “sicker” and thus had a higher risk of mortality. Residual confounding may also influence these outcomes. Conducting RCTs is essential for more definitive conclusions.
Regarding the procedural aspects of MT, in this study, the subgroup analysis of the MT group suggests potential insights into the technical aspects of MT for M2. Most cases required a combination of stent retrieval and aspiration techniques, reflecting the complexity of these distal occlusions. Furthermore, multiple thrombectomy attempts were often required, with nearly 61% of cases requiring three or more passes. This may highlight some challenges associated with navigating and recanalizing these small intracranial vessels. However, given the limited sample size, these observations should be interpreted cautiously and may warrant further investigation in larger studies.
While providing initial insights into MT for the M2 segment of MCA occlusions, this study has several limitations. First, the limited sample size constrains the statistical power and generalizability of our findings. Second, the non-randomized, observational design introduces potential selection bias and confounding variables. Third, there is a possibility that patients selected for more aggressive interventions like mechanical thrombectomy had different baseline clinical characteristics, potentially influencing outcomes independently of the treatment effect. Fourth, the absence of perfusion imaging due to resource constraints limits our ability to assess cerebral blood flow comprehensively. Fifth, the study lacks a direct comparison to intra-arterial thrombolysis and does not explore the impacts of precise lesion location, collateral circulation, or time to revascularization. Finally, the absence of long-term follow-up beyond 3 months restricts our understanding of the sustained effects of the treatments. These limitations underscore the need for cautious interpretation of our findings and highlight the importance of future RCTs in establishing causal relationships and more effectively controlling for potential confounding factors.
To address these limitations, future large-scale, multicentre RCTs with perfusion imaging, particularly perfusion mismatching, are recommended to validate findings, compare endovascular treatment modalities, identify predictors of successful recanalization and favorable outcomes, refine patient selection criteria, and optimize treatment strategies for M2 occlusions to help improve patient outcomes. Such trials would provide more robust evidence to guide clinical decision-making in managing M2 MCA occlusions.




留言 (0)