
記住我



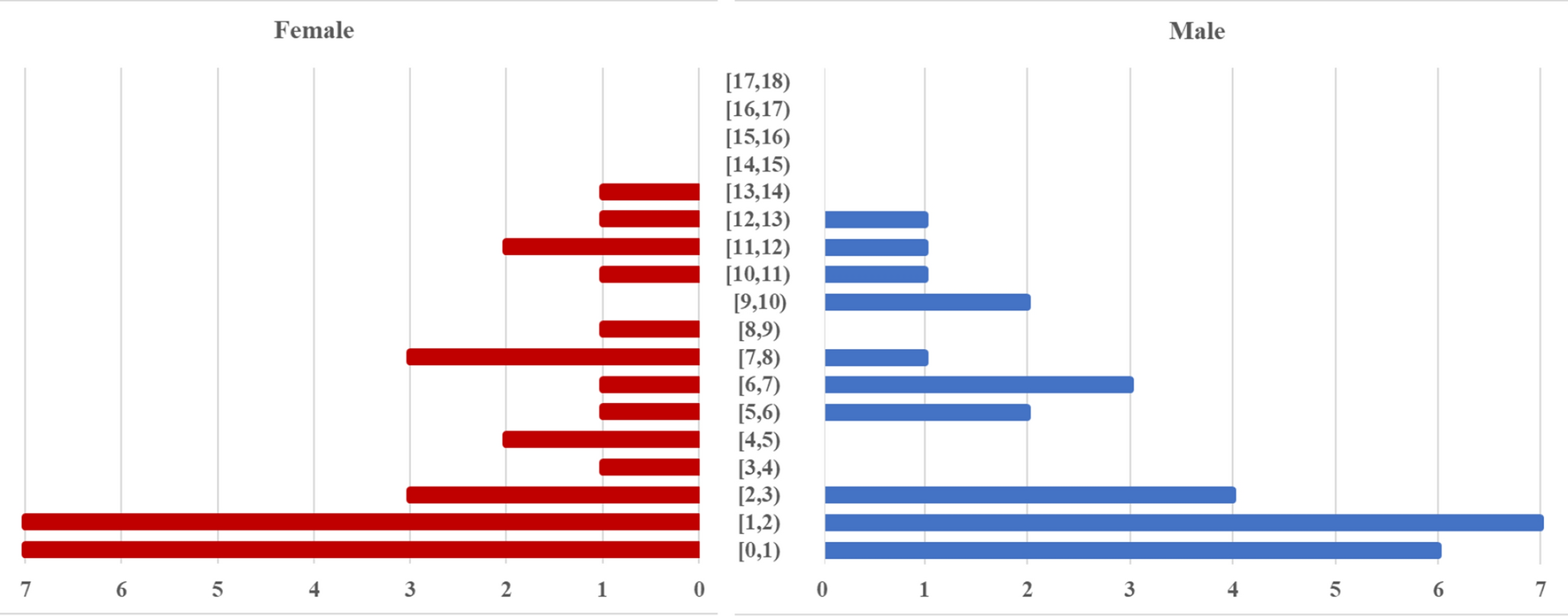
This study involved 17 patients who were being evaluated for ischemic events in the vertebrobasilar system. Of the participants, seven were females (41.2%) and ten were males (58.8%). The age range was from 35 to 76 years, with a mean age of 58.47 ± 9.41 years. The most prevalent comorbidity was a previous transient ischemic attack (TIA) in 15 patients (88.2%). This was followed by hypertension (HTN) in 12 patients (70.6%), and diabetes mellitus (DM) and hyperlipidemia in 10 patients each (58.8% for both). Ischemic heart disease was present in 6 patients (35.3%), while smoking was reported by 5 patients (29.4%), Table 1.
Table 1 Demographic and clinical criteria of the studied patientsThe primary location of stenosis was intracranial in 11 patients (64.7%), with extracranial being the second most common site in 6 patients (35.3%). In addition, the main stenotic artery was identified as the basilar region in 7 patients, accounting for 41.2% of cases. The proportion of patients with stenosis exceeding 70.0%, as determined by computed tomography angiography (CTA) was 12 patients (70.6%), while by digital subtraction angiography (DSA) it was 14 patients (82.4%). Five patients (29.4%) were classified as Mori type A, while 3 patients (17.6%) as type B and another 3 patients (17.6%) as type C. The most common cause of stenosis observed was atherosclerosis, affecting 11 patients (64.7%). This was followed by dissection, which was observed in 6 patients (35.2%), Table 2. Sixteen patients (94.1%) underwent general anesthesia, while one patient (5.9%) underwent local anesthesia. Access was primarily through the femoral artery in 15 patients (88.2%), with radial and brachial access used in one patient each (5.9% each). Pre-dilatation was not performed in 11 patients (64.7%), while it was performed in six patients (35.3%). The Resolute Onyx DES stent was used in 16 patients (94.1%), and the Neuroform Atlas stent was used in one patient (5.9%). After stenting, 15 patients (88.2%) had no residual stenosis, one patient (5.9%) had residual stenosis less than 10%, and one patient (5.9%) had residual stenosis less than 50%. No peri-procedural complications were noted in 16 patients (94.1%), while one patient (5.9%) experienced intracerebral hemorrhage, leading to death. Over all, the procedure was successful in 15 patients, which means stenosis improvement with no peri-procedural complications (88.2%), and unsuccessful in 2 patients (11.8%), Table 3. The MRS score was significantly decreased after a 3-month follow-up compared to the pre-operative scores. The interquartile range (IQR) changed from (1–3) to (0–2), respectively, with p value of 0.024, Table 4. There was no statistically significant difference found between extracranial and intracranial stenosis in terms of the final outcome. In extracranial stenosis six patients (100.0%) showed successful outcome. While in intracranial stenosis nine patients showed no complications (81.8%) which was not statistically significant with a p value of 0.266. Similarly, there was no statistically significant difference found between extracranial and intracranial stenosis in terms of residual stenosis. Six patients (100.0%) in extracranial stenosis had no residual stenosis. While in intracranial stenosis nine patients (81.8%) had no residual stenosis, which was not statistically significant with a p value of 0.446. Furthermore, there was no statistically significant difference found between extracranial and intracranial stenosis in the incidence of peri-procedural complications. In extracranial stenosis none of patients (0.0%) experienced peri-procedural complications, while in intracranial stenosis, one patient had intracranial hemorrhage (9.1%) which was not a statistically significant with a p value of 0.446, Table 5.
Table 2 Radiological characteristics of the stenotic vertebrobasilar stenosisTable 3 Peri-procedural outcomesTable 4 Follow-up for MRS at different times of measurement among the studied patientsTable 5 Relation between site of stenosis and postoperative outcomesCase 1A 58-year-old male with a history of diabetes, smoking and ischemic heart disease. He was scheduled for coronary artery bypass grafting. He presented with dizziness and syncope. MRI imaging showed a small area of infarction in the left cerebellar hemisphere. Angiography revealed significant stenosis in the proximal basilar artery. The patient underwent a successful stent angioplasty of the basilar artery, Fig. 1.
Fig. 1
Pre (A, B) and post (C, D) stenting of proximal basilar stenosis
Case 2A 65-year-old female patient with hypertension, diabetes mellitus, ischemic heart diseases, and dyslipidemia presented with TIA with manifestation of right sided weakness and ataxia. CT brain revealed a left cerebellar infarction (DSA) was performed, showing stenosis greater than 90% of the mid basilar artery and 50% stenosis of bilateral V4 segment of vertebral arteries. Stenting and angioplasty of basilar lesion were uneventful and vertebral stenosis was considered for medical treatment, Fig. 2.
Fig. 2
Pre (A, B) and post (C, D) stenting of mid basilar stenosis
Case 3A female patient 65 years, with past history of hypertension, DM and dyslipidemia, presented with TIA, right-sided weakness, and ataxia. CT brain showed left cerebellar infarction, DSA was done and showed dissection of the left VA with more than 90% stenosis. Right vertebral artery was totally occluded with no collaterals from both posterior communicating arteries. The first stent was deployed proximally as the stenosis was occlusive and the more distal lesion was not seen before the proximal stent then another stent was deployed to cover the distal lesion only. Decision was made to stop at this point as no flow limiting lesion was seen and to keep the left vertebral more mobile, Fig. 3.
Fig. 3
A Left vertebral artery dissection. B First stent was deployed proximally as the stenosis was occlusive and the more distal lesion was not seen before the proximal stenting. C Another stent was deployed to cover the distal lesion only Decision was made to stop at this point as no flow limiting lesion was seen and to keep the left vertebral more mobile. D, E First and second stent deployment. F Fluoroscopic AP view of both stents. G Successful recovery of VBS circulation
留言 (0)