
記住我








In the period 1.1.2021–31.1.2021, the Clinical Genetics services were operating in six areas of the region, employing a total of 25 certified clinical geneticists (22.4 Full Time Equivalents, FTE, corresponding to an average of 0.54 FTE every 100.000 inhabitants, see also Table 1), together with 43 FTE Clinical Scientists (Biologists/Biotechnologists), 35 FTE lab technicians, 11.4 FTE Nurses, 5.9 FTE Administrative staff and 4.1 FTE other support staff (Fig. 1). The seventh service, initially involved, was not included in the calculations since it is a specialized center for skeletal diseases and is not directly associated to a specific geographic area. As explained in the Methods section, medical residents were excluded from the official count: nevertheless, in order to have a more comprehensive overview, we report that, in the same time frame, a total of 17 residents (not shown in Table 1; Fig. 1) were participating in genetic counseling throughout the training network.
Fig. 1
Composition of the staff of the six clinical genetics services (FTE = Full Time Equivalent). The absolute numbers are inside the colored bars, while percentage is on the y-axis. The codes on the x-axis indicate the different clinical genetics services. As explained in the text, medical residents and staff from highly specialized centers were excluded
Table 1 Number of professionals involved in genetic counseling related to the population (MD = medical doctors specialized in Clinical Genetics, residents are not included)Three of the centers (C03, C05, C06) belong to academic hospitals and contribute to teaching activities of Medical, Nursing, Biology and Biotechnology Schools. Moreover, two of them (C05, C06) coordinate Postgraduate Residency Programs of Medical Genetics, whereas all the hospitals participate in the Residency network, hosting variable numbers of clinical geneticists in training.
While all the clinical geneticists are involved in genetic counseling, involvement of other professionals, namely clinical scientists and nurses, is still limited. Selected biologists are performing short pre-test genetic counseling sessions for screening tests (e.g. cystic fibrosis or karyotype in IVF programs) in C01, C02 and C03. Nurses mostly collaborate for sample collection and patient registration, but they are actively employed in selected genetic counseling sessions (e.g. pre-testing genetic counseling in karyotypic analysis) in some centers (C04, C05, C06).
WorkloadIn 2021, a total of 14,925 genetic counseling sessions have been delivered by the clinical genetics services of Emilia-Romagna, including both the consultations for new patients and the follow-up visits (see Limitations). It can be approximated that most of them are new patients, since follow-up visits are only prescribed for selected patients who previously underwent genetic testing.
In terms of time, the average annual clinical workload per physician is 1166 h, with an average of 14.5 consultations per week. Approximately one out of 278 inhabitants in Emilia Romagna received a genetic consultation in 2021 (Table 2).
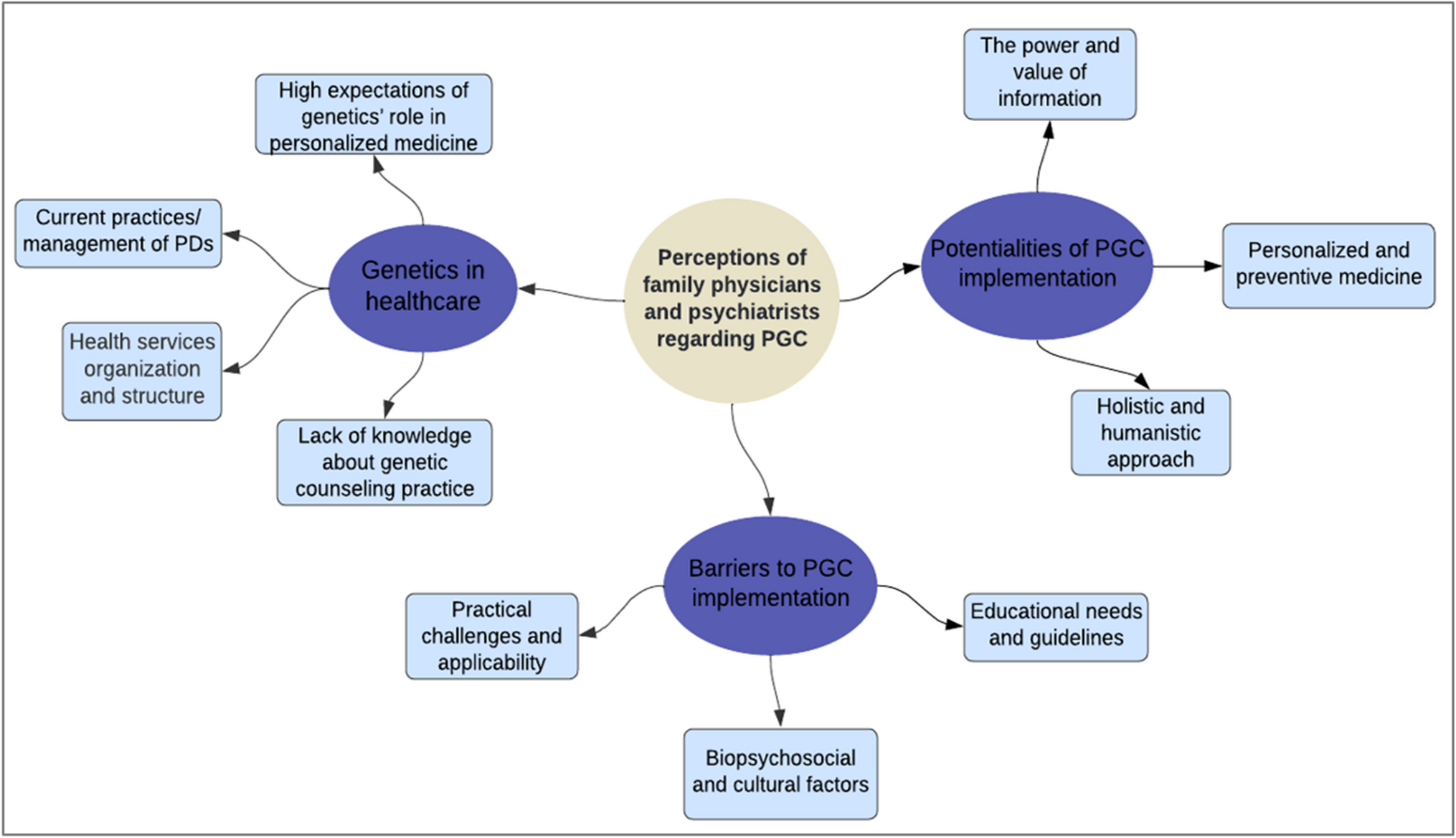
Table 2 Number of genetic counseling sessions compared to the medical staff* and the inhabitants of the six areas covered by the clinical genetics services in Emilia-Romagna (*Other healthcare professionals were not included in this calculation because their work in this context is under MD responsibility)Qualitative phaseThe directors of five out of six Clinical Genetics services agreed to participate in the Focus Group: four (C01, C03, C04, C06) in-person, the other one (C03) online through the Teams platform. As reported in Fig. 2, the discussion revolved around the following major themes (Fig. 2):
1.Access to genetic services.
2.Organization of clinical activities.
3.Interaction with health professionals from other disciplines.
4.Issues related to Service staffing and infrastructure.
Fig. 2
Results of the qualitative analysis
Access to genetic servicesIn the focus group, access to genetic services was discussed, with special regard to the opportunity of screening requests and pre-select clients for whom genetic evaluation is appropriate and clinically useful.
Indeed, a meaningful proportion of referrals is regarded as not appropriate, which impacts on the efficiency of services; this seems particularly common among self-referrals:
…at least half of self-referrals for cancer genetic counseling are inappropriate….
…there are people requesting counseling because they have been diagnosed with celiac disease and Hashimoto thyroiditis […] I wonder whether it has been explained by gastroenterologists and endocrinologists [that those are not mendelian diseases]….
Among participants, two reported to systematically perform preliminary evaluation of the requests to select those that are appropriate, while in the other services the selection is not standardized or is limited to specific request types (urgent prenatal consultations).
Triage may be performed through a structured way, with self-referring patients required to fill in specific forms and provide clinical documentation:
… each geneticist oversees a subspecialty clinic (pediatrics, cancer, etc.) and assesses respective request forms and clinical documentation….
Alternatively, requests are discussed in staff meetings, but assessment is made by an expert of the subtype as well:
We assess the requests every Friday morning. Each of us has expertise in one specific field….
Even in the absence of a triage procedure, the clinical geneticist is often requested to confirm the appropriateness of the referrals:
When the secretary is unsure, she asks the nurses, who eventually ask me… it does not work properly; nurses should be more autonomous in triaging cases….
In C06, where triage is applied, patients who do not meet requirements for accessing consultations receive remote genetic counseling by a clinical geneticist:
… if a request is not appropriate, we call the person by phone […] every month, one of the clinicians – yes, unfortunately a physician – is on turn for telephone counseling. We then report in the hospital platform the reason why we did not deliver the consultation requested….
‘…we perform a videoconsultation…’.
In several services, a proportion of appointments for genetic consultations is made through a centralized booking system (“CUP”) of the area, which citizens use to arrange medical examinations without any prior selection.
Organization of clinical activitiesAnother theme of discussion was the organization of clinical activities: a relevant impact of variable complexity and time-length of different consultation types were generally acknowledged:
Sometimes a consultation takes one-hour, other times two hours, then you have to study the case further […] many are complex consultations, especially the pediatrics ones!
…in consultations on reproductive matters, there are two consultants for one visit, and you need to collect both pedigrees.
…those planned by CUP [centralized booking system] are more likely to be inappropriate requests, and need no more than 15 min….
The complexity of consultations is not paralleled by adequate financial recognition in the public healthcare system:
…the fact that there are only two fares (first consultation and follow-up), both very low, means that complexity and time-consumptionn are not properly valued!
Timing of clinical report provision was also a matter of discussion:
‘We check the clinical records before the consultation and prepare a draft […] however after examining the patient a differential diagnosis may be needed, implying much more work to study the case; we may give the family a provisional report, or waiting to have completed the evaluation to give the final report’.
Among the strengths of the organization, the co-existence with a genetic laboratory allowing multi-professional case discussion and the ability to offer various types of consultations, with dedicated clinics, were reported:
…the implementation of dedicated clinics is progressively increasing and reflects the multiplication of medical branches interacting with the Genetics: this is the evolution….
Interaction with health professionals from other disciplinesA relevant part of the focus group was pointed on the interaction with health professionals of other disciplines; issues raised included proper referral, awareness/perception of genetics/geneticists and establishment of multidisciplinary paths.
Beyond self-referrals, even referrals from other specialists may pose issues:
…some cardiologists refer hundreds of elderly patients with cardiomyopathy [occupying all the available slots], then complain because the first appointment available for a 30-year-old patient is after one year….
Nevertheless, the issue of what types of consultations should be deemed as appropriate was raised in the discussion, eliciting different views.
Someone was in favor of broader access criteria:
A person who is worried because of a family history of colon cancer has the right to receive counseling.
…even for a common condition such as autism, clinical genetic assessment may reveal clues for a syndrome diagnosis, so it is preferable to see as many cases as possible….
Others would prefer stricter selection:
‘For very common situations, other health professionals should be in charge of giving proper information […] our role should be to promote knowledge and raise awareness, not to deliver counseling to each individual’.
In any case, instances of scarce awareness about the role of geneticists and the complexity of genetic tests among other specialists were unanimously reported:
‘Cardiologists and Neurologists may be surprised by the time-lapse between referral and test results; after seeing patients and refer them for a genetic consultation, they expect that results of genetic investigations are immediately available for them to conclude their assessment’.
‘There is not yet enough knowledge of our discipline’.
However, it was suggested that working together with geneticists in multidisciplinary paths may lead other physicians to recognize their role and the added value of integration:
‘At the beginning many clinicians do not understand our role: genetic counseling seems an unnecessary step, which complicates and delays the route to genetic testing; later on, when they have to face challenges in clinical interpretation of test results, communication to other family members and so on, they recognize the value of our discipline: we need to interact more to change their mind, their prejudices’.
The value of multidisciplinary paths was recognized by all participants; someone highlighted the value of joint clinics and multidisciplinary assessment of patients:
…often children need to be seen by clinical geneticists and neuropsychiatrists together, otherwise some diagnoses may be missed….
We run a joint clinic with Gastroenterologists for individuals at familial risk of digestive cancers: even if there are no criteria for genetic testing, they can enter a surveillance program….
‘We meet on a regular basis with every multidisciplinary team we have joined’.
For some disorders, mainstreaming approaches were deemed highly efficient:
…we must collaborate with other specialists […] there is no reason for us to see every single patient with pheochromocytoma, who undergoes genetic testing in any case.
‘We should establish multidisciplinary paths and work mostly in integrated care pathway sharing criteria for genetic testing, which can be arranged by other specialists: we should see only patients with variants detected or with suspicious features and discuss complex cases in multidisciplinary meetings’.
Issues related to service staffing and infrastructureCompared to the number of consultations registered, perceived workload was much higher, since several activities, such as triage and telephone genetic counseling, that are carried out by clinicians fail to emerge in quantitative assessment; thus, all felt that the number of clinicians in the services is undersized for the work required:
Triage is energy- and time-consuming. It constitutes a heavy load for clinical geneticists.
Even one more doctor would be of help….
There is too little time for in-depth study of cases and for research….
Other staff is of limited help for genetic counseling activities:
For specific tests, pre-test counseling is targeted and is delivered by a clinical scientist, who provides clients with an information sheet and some explanations, but no more….
…our nurses oversee sample collection and mailing […] we would need nurses trained in genetics, who may contribute to counseling activities….
‘…we would need a specialized nurse to manage the cases…’.
Lack of administrative and technological support is felt to increase the non-clinical workload of physicians:
A lot of work is administrative in nature, and should be made by administrative staff, who in reality is largely inadequate in terms of numbers.
‘If we had more processive informatic platforms supporting clinical work, test requests, and so […] we would save time and energies…’.
留言 (0)