
記住我
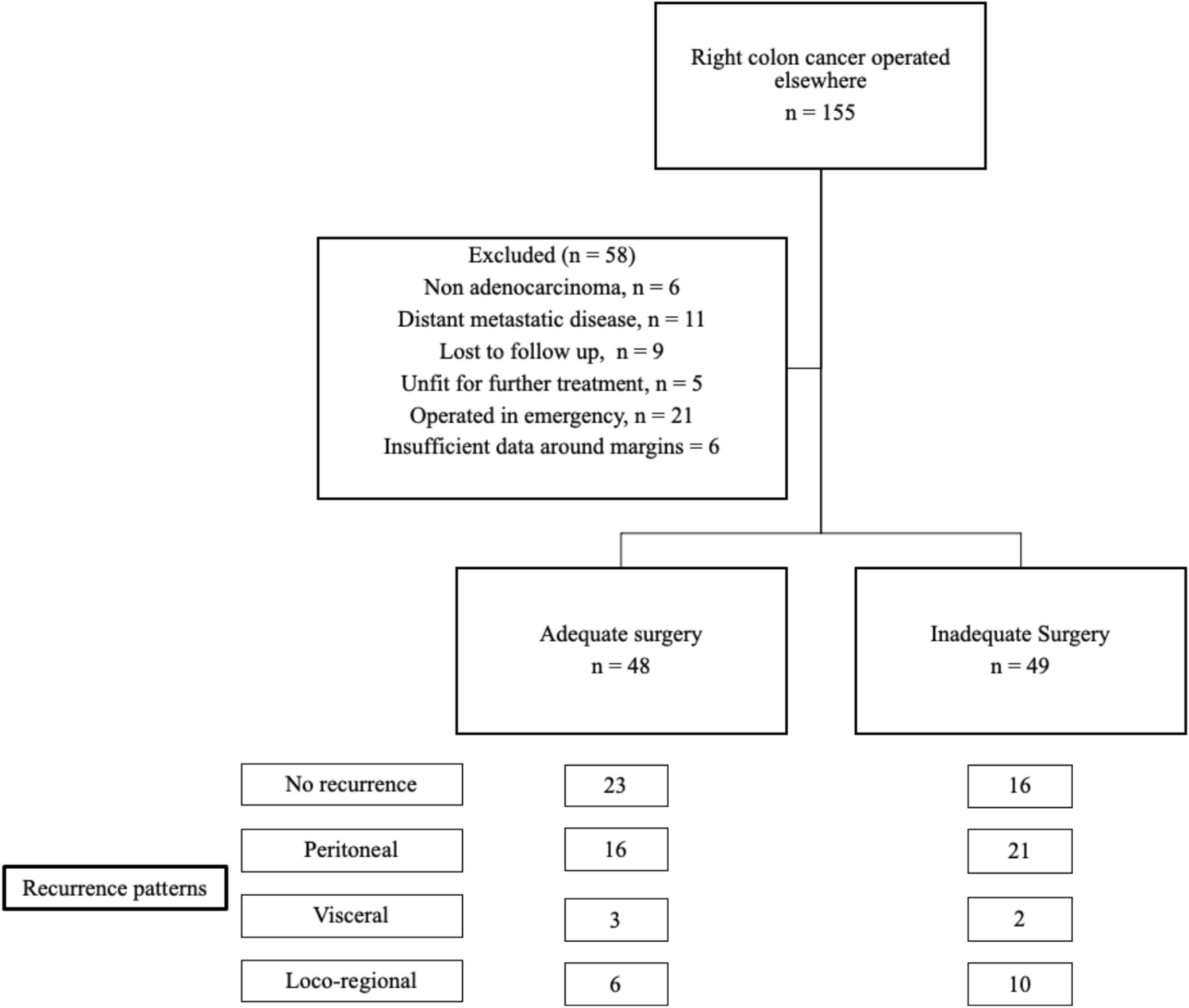

The current study analyzed the outcomes of patients undergoing inadequate surgery in a non-oncological setup and then subsequently managed with chemotherapy alone. At the end of 2 years, the OS of the cohort was 71.5% and the corresponding DFS was 45.8%. An alarming 58 out of 97 patients (59.8%) suffered early disease relapse (first 2 years), with peritoneal relapse being most common in 37 patients (38.1%). When patients had inadequate nodal harvest (less than 12 nodes), survival was similar between patients with lymph node metastases and negative lymph nodes. With the increasing harvest of lymph nodes, the group with lymph node metastases had progressively decreased survival in comparison to those with negative lymph nodes.
Hohenberger et al. introduced the concept of CME for right colon cancers, citing the number of lymph nodes dissected to be a surrogate of surgical adequacy [1]. They suggested retrieval of 28 lymph nodes as an adequate nodal harvest in right colon cancer. Upon dissection of more than 28 nodes, patients had significantly superior survival outcomes, irrespective of the involvement of nodes with metastatic disease. The concepts of CME with CVL and D3 lymphadenectomy propagated by the West and East groups of surgeons, respectively, aim at a higher nodal yield after radical surgery. In principle, the concept of CME and D3 lymphadenectomy proposes thorough clearance of the lympho-vascular packet while removing the central nodes. In the current study, authors hypothesized that inadequate clearance should lead to higher chances of peritoneal metastases secondary to tumour spillage caused by disruption of lymphatic channels, especially in those having metastatic regional lymph nodes. With this hypothesis in mind, this study is an attempt to shed light on the outcomes of patients who underwent inadequate index surgery in the community setting.
In a recent publication from the same institute, authors have elucidated the outcomes of patients with right colon cancers treated with CME and CVL at the institute [9]. Desouza et al. have shown that patients undergoing adequate right colon surgery have a 5-year OS and DFS of 87.5% and 80.4%, respectively. Thirty-seven of 244 (15.2%) patients suffered relapse at a median follow-up of 62 months, with peritoneal relapse being seen in 6.1% patients. Distant visceral metastases were the most common site of relapse (7%). Similarly, in other published literature, locoregional and peritoneal recurrences are usually seen in 4% and 4.5% cases, respectively [10,11,12]. However, the current study reports peritoneal recurrences in 38.1% cases. This high rate of peritoneal relapse is alarming and probably has its basis in inadequate index surgery. Authors hypothesize that disruption of lymphatic channels during the sub-optimal surgery coupled with inadequate nodal clearance leads to an increased risk of subsequent peritoneal relapse.
This high rate of peritoneal recurrence points to an unrealized need for treatment intensification upon referral to a tertiary centre. Currently, the treatment options available for such patients presenting after an initial sub-optimal surgery include either a revision completion surgery or chemotherapy. Although there are no published reports on the management of the same, patients are usually offered chemotherapy. The main reason for deferring a revision surgery is a technically challenging dissection around the mesenteric-portal axis in an already operated surgical field.
None of the published studies have analyzed the actuarial benefit of chemotherapy in patients with incomplete primary surgery. It is unclear if chemotherapy alone could compensate for a sub-optimal surgery. Authors suggest that the practice of chemotherapy after an incomplete surgery seems more convenience-based, rather than evidence-based.
Surgery with R-0 resection offers the only chance at long-term cure of locally recurrent colon cancers [13, 14]. While such operative strategies have been shown to improve outcomes in recurrent settings, similar treatment schema may lead to improved outcomes in patients after an index incomplete surgery by removing microscopic or macroscopic residual disease. This may especially hold true for the subset of patients who are found to have radiological residual disease upon restaging at presentation. In the current study, a sub-group of patients with residual disease were found to have significantly inferior OS and DFS as compared to patients with no residual disease. Authors postulate that delaying revision completion surgery in patients with radiological residual disease with chemotherapy first approach results in increased rates of unsalvageable peritoneal metastases. In this study, only 15.5% recurrences were surgically salvageable.
Treatment and referral pathways for colorectal cancers (CRCs) have been standardized in the West [15,16,17]. However, a similar standardization is lacking in low-middle-income countries (LMICs). This leads to an increased burden of inadequately treated colon cancers in LMICs. While the debate continues on the aggressiveness of lymphadenectomy in per-primum cases, operative strategies need to be defined and standardized for sub-optimally treated right colon cancers. This definition of an alternative treatment strategy for inadequately treated colon cancer is the need of the hour, especially in those countries where referral patterns are not standardized.
The current study shows that the OS of the overall cohort was 71.5%, and the corresponding DFS was 45.8% at the end of 2 years. This is very low compared to the reported outcomes after adequate treatment of colon cancers [18]. In such cases, when the reported outcomes are inferior, especially in patients with residual disease after primary surgery, the option of alternative treatment (revision surgery) should be discussed with the patients.
In this study, amongst patients with less than 12 lymph nodes harvested, patients with no lymph node involvement had similar survival as patients with involved lymph nodes. Amongst patients with 12 to 27 nodes dissected, patients with no involved nodes had significantly superior OS and DFS. Amongst patients with more than 28 nodes dissected, there were no events during the study period with significantly increased OS and DFS. Authors propose a role for revision surgery at presentation in patients with less than 12 nodes dissected at index surgery. Patients with more than 28 nodes dissected may be safely placed on routine follow-up after completion of chemotherapy. In the intermediate group (12 to 27 nodes), it may be wise to have a discussion with the patient for revision surgery versus observation after completion of chemotherapy (Fig. 3). Segregation of patients based on lymph node dissection and residual disease into varying treatment strategies (revision surgery or only chemotherapy) may provide a plausible solution to improve the disease outcomes.
Fig. 3
Suggested treatment algorithm for patients with an inadequate index colectomy
This study provides the first description of outcomes of colon cancers with an index inadequate colectomy, done in non-oncological setups in inexperienced hands. The authors acknowledge poor outcomes after such inadequate preliminary surgery. It is a hypothesis-generating study which lays emphasis on the role of revision surgery as a possible strategy to improve outcomes of sub-optimally treated colon cancers. Limitations of this study include its retrospective nature along with a limited sample size. The possibility of non-documented peritoneal disease at the preliminary exploration is noted and it may be a part of recall bias inherent to the retrospective study design.
Currently, there is a lack of evidence to support the role of revision surgery in decreasing the rate of peritoneal metastases. Further trials comparing the role of adjuvant chemotherapy alone versus upfront revision completion surgery for such patients would provide the appropriate solution to the problem at hand. This study may serve as a basis for the calculation of appropriate sample size for such trials in the future. Specialized surgical units dealing with recurrent right colon cancers need to standardize the often technically challenging dissection along the mesenteric-portal axis while avoiding serious morbidity. The addition of intra-peritoneal chemotherapy during relook surgery to these patients being explored after an inadequate colectomy may be another potential area of research.
留言 (0)