
記住我






This is a population-based retrospective multicenter study on registry-based data from patients with diagnosed rAAA within Stockholm County, from 2010 to 2021.
The Stockholm County region had a population of 2.3 million inhabitants (2019). There are seven hospitals with emergency medical care units, of which two provide elective and emergent vascular surgery for the whole region in a combined on-call service (Karolinska University Hospital and Stockholm South General Hospital). All patients in the region with vascular emergencies are admitted or referred to one of these two centers, approximately 55–59% of all vascular patients will be admitted to the Karolinska University hospital. There is always a vascular surgeon on-call for vascular emergencies working at this hospital. Patients with or without verified rAAA deceased at other hospitals, that are not referred are not included.
Study cohort and definitionsThe cohort was extracted by two means; from the Swedish National Registry for Vascular Procedures, Swedvasc [3], which registers all vascular interventions performed at the Karolinska University Hospital since 1994 with an external validity of (98–100%), and the in-hospital registry for diagnosed rAAA patients, including all rAAA patients admitted to the Karolinska University Hospital, thereby also catching all admitted but untreated patients with certified rAAA. Figure 1.
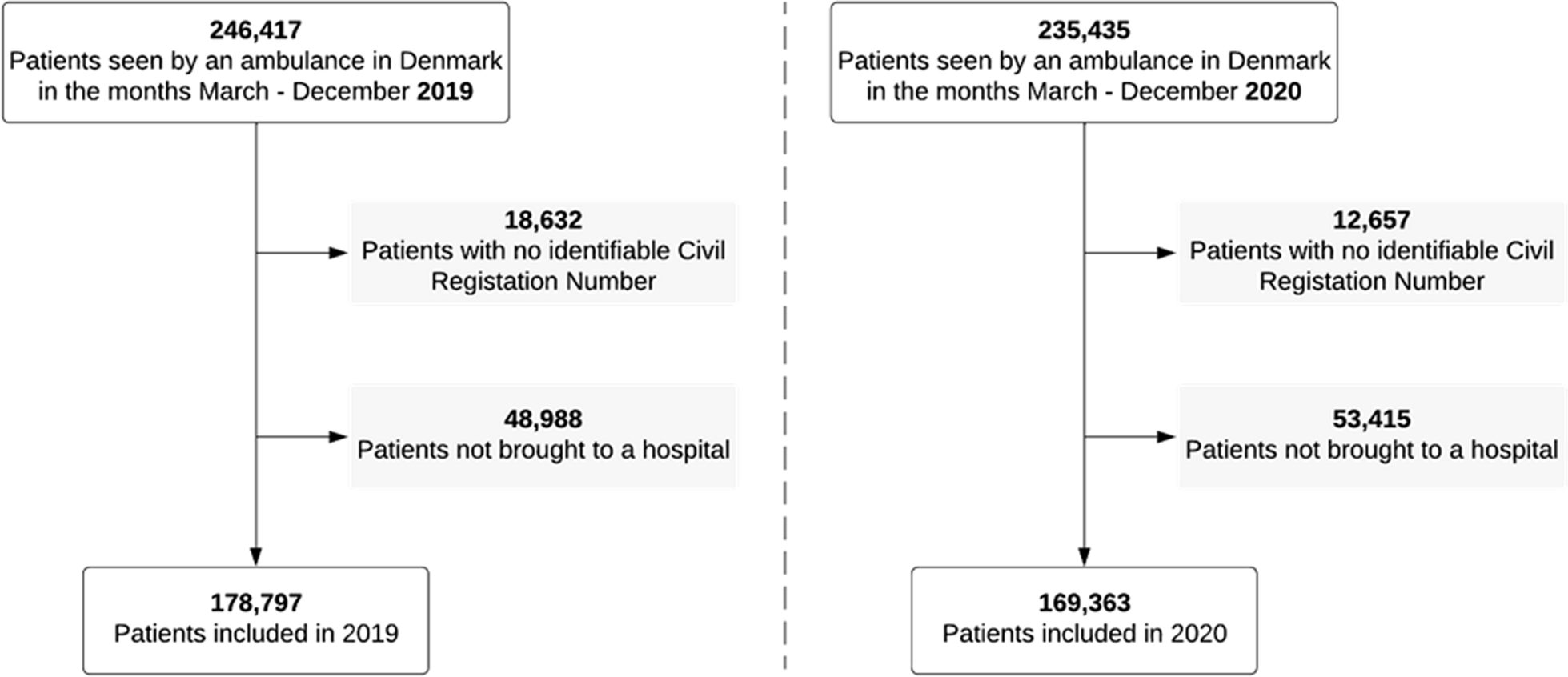
Fig. 1
Flow chart of included patients with ICD code I71.3, based on the primary cohort of infrarenal rAAA cohort identified through the EMR, selection, exclusion, and inclusion criteria
Patient Identity Number (PIN) and data from all patients with verified rAAA, untreated or treated with either open or an endovascular aortic repair were collected. A total of 277 patients were identified from January 2010 to October 2021 in the Karolinska University Hospital (Fig. 1). Patients diagnosed with rAAA not selected for vascular intervention were identified through the international classification of disease-10th edition (ICD-10), which uses ICD-code I71.3 for verified rAAA, at Karolinska University Hospital. A total of 276 patients were identified using Swedvasc registry and the Karolinska hospital electronic medical records (EMR).
This leaves one missing patient with a rAAA-diagnosis, lacking a clear description of care or treatment. Conservative treatment with palliation was chosen for 16 patients. After exclusion of non-infrarenal aortic ruptures, a total of 216 patients were identified and included (49 women and 167 men). In total, sixty patients were deemed not eligible for inclusion (Fig. 1).
Data was collected regarding comorbidities and risk factors for vascular disease as registered in any note in charts, any time prior to the event of rupture. Weight and height were commonly provided in the EMR. Radiological findings, i.e., computer tomography and, or ultrasound at admission were registered.
Clinical symptoms (abdominal, back, flank, groin and chest pain, dizziness, syncope, nausea, vomiting, dyspnea, pulsatile abdominal mass) were registered as stated in the EMR.
Dizziness was expanded in this study to include terms such as “about to faint”, “pale” and cold/shivering since it was commonly described and in general terms were evaluated as equivalents to dizziness in this study.
Modified abdominal aortic aneurysm rupture signs, MARSThe current standard rAAA triad of signs include abdominal pain, syncope and pulsatile mass. The developed and proposed Modified-Abdominal Aortic Aneurysm-Rupture-Signs or MARS builds upon the current triad and includes the following:
All registries of pain (abdominal, back, flank, groin or chest) were included to “associated pain”. Similarly, syncope, dizziness, nausea, vomiting and dyspnea were sorted as surrogate symptoms indicating and related to “hypovolemic symptoms”. The clinical examination of the abdomen, which can indicate a pulsatile abdominal mass, can be enhanced by adjunct use of an aortic ultrasound, with transversal or longitudinal axis measuring the maximum infrarenal aortic diameter. This can be performed in the prehospital setting or at the emergency department (Figs. 2, 3). Most of the patients in this cohort were examined in the ER.
Fig. 2
Summary and prevalence of symptoms for STS and MARS. Standard triad consist of abdominal pain, syncope and pulsatile abdominal mass. MARS includes all registries of any localization pain, expression of hypovolemic signs and addition of sonography or examination of pulsatile abdominal mass
Fig. 3
Comparison of the Standard triad of signs (STS) to Modified-Abdominal-Aortic aneurysm Rupture-Signs (MARS). *Comparison of 2 and 3 signs for STS vs MARS and 3 signs for STS vs MARS (P value < 0.001)
StatisticsContinuous variables are reported as mean ± standard deviation or median and IQR (25–75 percentiles) depending on normal distribution tested with Shapiro–Wilk. Categorical data are presented using numbers and proportions. Statistical significance was tested for continuous data with Mann–Whitney U-test or t-test and for categorical data with Fisher’s test or Chi square depending on the number of patients. Two-tailed P value less than < 0.05 was considered significant. Statistical analysis was performed with IBM SPSS version 29.
留言 (0)