
記住我

This is a randomized controlled trial which will be carried out in three community-based psychiatric rehabilitation centers under the Singapore Anglican Community Services (SACS). The three centers are: Anglican Care Centre (ACC) Simei, ACC Hougang and ACC Bukit Batok. These centers provide standard psychiatric rehabilitation services for mental health clients with various psychiatric diagnoses. The clients are outpatients and live either within the community or in supported housing within the centers.
Adult clients (21 to 60 years old) who meet the following inclusion criteria will be recruited by the study team:
A diagnosis of schizophrenia or schizoaffective disorder according to the Diagnostic and Statistical Manual of Mental Disorders-5th Edition (DSM-V).
Completed at least ten years of formal education with English as the main instructional language. Participants need to be able to converse in English and understand English instructions, as the cognitive remediation program will be conducted in English.
The exclusion criteria are:
Known neurological diseases and epilepsy, which affect gains from cognitive remediation.
Unable to speak and understand English.
Hospitalized within the past one month.
Global Assessment of Functioning score of 30 or below, as participants who are too low functioning are unable to benefit from a metacognitive strategy learning approach.
Existing clients at the centers who meet the criteria will be approached by the research team to participate in this study, using IRB approved consenting procedures. The research team member will use the Participants Information Sheet to explain the research procedures and seek informed consent. The clients will be given an opportunity to ask questions and clarify their doubts. They will also be given time to think through before consenting. They will be informed that participation is voluntary and that they can withdraw from the research at any point in time, without affecting their psychiatric rehabilitation. Ethics approval has been obtained from the Singapore Institute of Technology Institutional Review Board (approval number: RECAS-0306).
Upon informed consent, the client will be enrolled as a research participant and the research assistants will administer the baseline measurements described in the subsequent section. Randomization will be done by the Principal Investigator using a computer randomization generator. All eligible participants will be randomly assigned to the experimental arm (cognitive remediation using adapted NEAR and standard psychiatric rehabilitation), or the control arm (standard psychiatric rehabilitation only) based on a 1:1 treatment allocation.
Study procedure and study conditionsUpon assignment to their study condition, the participants will commence their cognitive remediation and psychiatric rehabilitation (experimental arm) or standard psychiatric rehabilitation (control arm). SACS professional staff will undergo 36 hours of training to conduct the cognitive remediation. They will then deliver the cognitive remediation in their centers.
Experimental Arm- Cognitive Remediation: Metacognitive Strategy Based Neuropsychological and Education Approach to Remediation (NEAR)NEAR employs an integrated theoretical framework drawing from neuropsychology, educational psychology, behavior learning theory, and motivation theories [5]. It entails building a library of carefully chosen computer cognitive games to enhance cognitive performance through practice and strategy acquisition. This study will use a variety of web-based computer activities that have been used with NEAR in global contexts [32]. The metacognitive method of strategy learning will be informed by the Multicontext Treatment Approach. It encompasses mediation by the therapist to appraise the activity prior to engagement, identify error patterns and generate strategies during activity engagement, and reflect on the efficiency of the strategy used upon activity completion. Participants will also learn to monitor and regulate their motivation using strategies. Besides cognitive game sessions, bridging groups will be conducted to enable application of strategies to real-life situations encountered during psychiatric rehabilitation and in the participants’ living environment.
NEAR will be delivered three times a week for 12 weeks at the centers. The duration of each session within the week is as follows:
First session: 45 min computer-assisted cognitive exercises + 30 min bridging group.
Second session: 30 min computer-assisted cognitive exercises + 45 min bridging group.
Third session: 45 min computer-assisted cognitive exercises.
In total, there will be 36 sessions. Participants who miss a session will do make-up sessions and will complete the program over 12 weeks or slightly beyond. The NEAR fidelity checklist will be used to ensure adherence to intervention protocol.
Computer-assisted cognitive exercisesBased on the results of the baseline assessments, the therapist will complete a Cognitive Remediation Treatment Plan together with the participant. The treatment plan will outline the cognitive domains that the therapist and the participant want to target in the initial phase, the possible computer-based cognitive exercises and the possible therapeutic strategies that the therapists can deploy. Very importantly, the therapist and the participant must establish a functional goal that the participant wants to work towards. The functional goal will be based on the results of Canadian Occupational Performance Measure as described later.
The computer-assisted cognitive exercises are conducted using carefully selected computer cognitive games to restore cognitive functioning through rehearsal and strategy learning. Rehearsal is through drill-and-practice to improve discrete cognitive skills, while strategy-learning aims to equip participants with strategies to overcome cognitive challenges in different functional contexts. The sessions are conducted in groups of six to ten participants and facilitated by two therapists [6]. The cognitive games may target discrete cognitive skills such as attention, working memory and emotion recognition or a combination of different cognitive domains. In accordance with NEAR principles, games that are contextualized (eg: working in a restaurant, grocery shopping, taking a road trip etc.) will foster greater self-determination than games that simply target discrete cognitive skills. Therefore, the top-down approach of cognitive training will be utilized by the middle phase of the intervention. In addition, the Multicontext Treatment Approach to metacognitive-based strategy learning will be carried out from the start of the computer-assisted cognitive exercises sessions. The therapist and participant will identify error patterns/cognitive performance problems and work on the use of strategies to overcome challenges faced during the computer games sessions [18]. The metacognitive framework of self-evaluation and activity mediation will also be utilized. During the engagement of cognitive exercises, the therapist will facilitate the participants to appraise tasks challenges (pre-activity), mediate during the engagement of task and do post-task reflection. Strategies acquired during a game can be applied across other games. For example, a participant may have applied the strategies of ‘visualizing items’ and ‘chunking’ in a cognitive exercise that requires the participant to learn items on a grocery list. Upon post-task reflection, the participant evaluates that ‘chunking’ is effective when he can categorize the long list of items. The participant will then apply this strategy on another game that requires him to take on the role of a waiter to remember food orders.
At the same time, the participants will also acquire metamotivation knowledge and skills in metamotivational monitoring and control. This involves facilitating the participants to self-evaluate before, during and after each task. During bridging groups, they will learn about the different types of motivation and are introduced to a tool called ‘Motivometer’, to self-appraise their interest, meaningfulness, confidence and empowerment to a task. This will be carried over to their computer-assisted cognitive exercise sessions. The therapist may prompt the participants to appraise their motivation when they show obvious interest and when they are observed to be less motivated. This is to prompt them to notice the difference in their motivation levels. During the task, the participants will learn to adjust strategies to work towards sustaining their motivation and achieving the task goal. After the task, the participants will then evaluate their performance, reflect on their motivation and strategies used, as well as self-generate alternative strategies for the future. Strategies for motivation may involve positive self-talk, recalling past successes, bringing to mind personal goals etc.
Bridging groupsTransfer of learning is facilitated through bridging groups, to generalize strategies learned during the computer-assisted cognitive exercise sessions to situations and contexts that occur during psychiatric rehabilitation, as well as in the environment that the participant lives in [7].
Bridging groups will be conducted twice a week and may involve psychoeducation, role plays and hands-on activities. The hands-on activities may include physical games, performing instrumental activities of daily living etc., so that participants can utilize strategies learned during the computer game sessions to their psychiatric rehabilitation activities, community living, work tasks and social interactions. Participants will also learn more about cognitive impairments and how lifestyle modifications (eg: sleep, physical exercise), managing their mood and social participation can affect cognitive performance. In addition, metamotivation exercises from the motivation skills training by Hansen and colleagues [25] will be incorporated. These exercises aim to facilitate participants in building awareness about their motivation levels through self- reflection and self-monitoring.
Participants in the experimental arm will attend NEAR in addition to their usual psychiatric rehabilitation activities at the centers. They will also continue with pharmacological treatment as prescribed by their psychiatrists.
Control arm- standard psychiatric rehabilitationParticipants in the control arm will attend their scheduled activities at their respective Anglican Care Center. The centers run a variety of activities to provide psychiatric rehabilitation for clients with serious mental illness. These may include vocational training such as training in a retail shop or café, instrumental activities of daily living training (eg: taking public transport, money management), psychoeducation, social skills training etc. Participants in the control arm will not be enrolled into cognitive remediation but will continue with pharmacological treatment as prescribed by their psychiatrists.
MeasurementsThe Global Assessment of Functioning Scale (GAF) is used as a screening prior to recruitment to exclude clients who have a score of 30 or lower, since participants with very low functioning may not benefit from a metacognitive strategy learning approach. GAF is a numeric scale (0 through 100) used to rate symptom severity and social, occupational and psychological functioning of adults. The scale is indicated as Axis V in the Diagnostic and Statistical Manual of Mental Disorders-IV-TR and guidelines for scoring have been developed [33].
The following outcome measurements will be administered at baseline, post-intervention and eight weeks after intervention. These will be collected by research members who will not be implementing NEAR, so that outcome assessors are blinded to treatment allocation. Unblinding will not be carried out throughout the implementation of intervention.
Primary outcome measurementsBrief Assessment of Cognition in Schizophrenia (BACS): to assess neurocognition.The Brief Assessment of Cognition in Schizophrenia (BACS) assesses the aspects of cognition found to be most impaired and most strongly correlated with outcomes in persons with schizophrenia. This assessment was validated and found to be sensitive and highly correlated with the standard battery composite scores in patients (r = 0.76) and healthy controls (r = 0.90) [34]. BACS was also previously normed in English-speaking adult Singaporeans [35] and had demonstrated good convergent validity with education [36] and discriminability between healthy controls and schizophrenia [37]. BACS is now widely used as an outcome measurement for cognitive remediation.
Bell Lysaker Emotion Recognition Task (BLERT): to assess emotion processing (social cognition)The Bell Lysaker Emotion Recognition Task (BLERT) measures the participants’ ability to process and recognize seven emotional states: happiness, sadness, fear, disgust, surprise, anger, or no emotion [38]. The participants will be presented with 21 video clips of an actor demonstrating facial, voice-tonal and upper-body movement cues, while engaging in work-related monologues. Unlike static photos, this measurement appears to simulate real-world situations better and may approximate real world functional outcomes [39]. Rating is done by computing the total number of correctly recognized emotions (ranging from 0 to 21).
The BLERT was identified by the Social Cognition Psychometric Evaluation (SCOPE) workgroup as one of the three social cognitive outcome measurements with the strongest psychometric properties across all the six evaluation criteria: test–retest reliability, utility as a repeated measure, relationship to functional outcome, practicality and tolerability, sensitivity to group differences, and internal consistency [39]. The BLERT was also examined for its psychometric properties in a Singapore sample of outpatients with schizophrenia [40]. This was evaluated alongside a suite of social cognitive measures similar to the SCOPE study. BLERT was again identified as one of two social cognitive measures to be the most favorable, with little evidence of floor/ceiling effects and better tolerability ratings [40].
Social and Occupational Functioning Assessment Scale (SOFAS): to assess functioningThe Social and Occupational Functioning Assessment Scale (SOFAS) is a global rating of current functioning ranging from 0 to 100, with lower scores representing lower functioning [41]. It differs from GAF scale by focusing on social and occupational functioning independent of the overall severity of the individual’s psychological symptoms. SOFAS has been used as a functional outcome measurement in cognitive remediation trials [42,43,44].
Canadian Occupational Performance Measure: client-centered measurement of functional and personal recoveryThe Canadian Occupational Performance Measure (COPM) is a person-centered tool that measures aspects of functional and personal recovery among clients whose occupational performance and participation are affected by their current psychiatric conditions. Through a semi-structured interview, the clients identify activities in self-care, productivity and leisure that are of personal importance and rate their performance and satisfaction in each activity [45]. Self-perceived performance and satisfaction are rated on a 10-point Likert scale. As such, this tool measures the participants’ ability to fulfil valued life roles and to perform activities that are meaningful to them, which gives an indication of functional and personal recovery.
The COPM has been found to be applicable for community-dwelling persons with schizophrenia and is an appropriate tool for use in psychiatric rehabilitation and recovery-oriented services [46, 47]. It has good intraclass correlation coefficients and test–retest scores that range from r = 0.842 to 0.847 [48]. It enables clinicians and researchers to chart functional performance, level of satisfaction and inclusion in clients’ daily lives.
Secondary outcome measurementsPositive and Negative Syndrome Scale (PANSS): to measure symptomatologyThis is a 30-item rating instrument that evaluates the presence and severity of positive, negative and general psychopathology of schizophrenia [49]. The scale was developed from the Brief Psychiatric Rating Scale (BPRS) and the Psychopathology Rating Scale. All 30 items are rated on a 7-point scale (1 = absent; 7 = extreme). PANSS covers positive and negative symptoms associated with schizophrenia, as well as other symptoms (eg: aggression, thought disturbance, depression). Its five-factor model structure has also been validated with persons with schizophrenia in Singapore [50]. Hence, the PANSS is a sound instrument to be used for symptom measurement.
Brief Negative Symptom Scale (BNSS): to measure negative symptomsBNSS consists of five domains of negative symptoms (anhedonia, asociality, avolition, blunted affect, and alogia), which could be clustered into two factors: Motivation-Pleasure (MAP) and Emotional Expressivity (EE) [51]. A validation study on outpatients with schizophrenia found that BNSS showed good internal consistency and validity [52]. In addition, more severe symptoms as shown in BNSS total, avolition and asociality domains were associated with lower scores on the Global Assessment of Functioning [52].
Brief Regulation of Motivation Scale (BRoMS)-adapted: to measure metamotivationMetamotivation is the self-regulatory processes by which individuals identify, monitor, and control their motivational states in alignment with their goals [53]. The Brief Regulation of Motivation Scale (BRoMS) was initially developed to assess college students’ regulation of motivation and two factors were identified: regulation of motivation and willpower [54]. Subsequently, a study that adapted and validated it for schizophrenia population found it to be acceptable, feasible and internally consistent, with higher BRoMs scores associated with better work-related skills [31]. The adapted BroMs is a structured interview where participants are told to identify three tasks that they have been working on during the past week. The tasks should require participants to maintain their effort over hours or days. The participants will then be given 12 statements, where they rate on a 4-point scale, from ‘Strongly Disagree’ to ‘Strongly Agree’ [31]. These statements are related to awareness and regulation of motivation, for eg: “If I feel like stopping before I'm really done, I have strategies to keep myself going”.
Weekly Calendar Planning Activity (WCPA)The Weekly Calendar Planning Activity (WCPA) is a performance-based measure of metacognition, that requires the participant to plan and execute a multiple-step activity. It involves scheduling a list of appointments into a weekly calendar while following rules, avoiding conflicts, monitoring time, and inhibiting distractions, thereby evaluating the participant’s planning, error recognition, use of strategies and self-monitoring [55]. Besides scoring for accuracy, the WCPA also scores the difference between the participant’s estimated performance and his/her actual performance. Hence, it also evaluates the participant’s self-awareness [56].
The WCPA has been used as an outcome measurement for persons with schizophrenia participating in metacognitive interventions [57]. It has high interrater reliability scores ranging from 0.94 to 0.99 and a high test–retest reliability [58].
To reduce test fatigue, the measurements may be administered over two sessions but within two consecutive days. Table 1 summarizes the list of outcome measurements and their schedule.
Table 1 List of scheduled outcome measurementsData management planEach participant will be given a participant number, and all participants’ demographics and outcome measurement data will be linked to their assigned number. Therefore, all data collection forms will only contain the participant numbers and no identifiers will be written. The collected data will then be transferred to a password-encrypted spreadsheet.
There will be two separate encrypted spreadsheets. The first spreadsheet will contain the participants’ demographic information and outcome measurements data. However, there will be no participant identifiers and only the participants’ assigned numbers will be indicated. The second spreadsheet will link the participant’s names to the participant’s assigned number and will only be accessible by the Principal Investigator using a different password.
A Data Management Plan has been approved by the university’s Applied Research Office, to access a secure Data Store SharePoint Folder. The password-encrypted spreadsheets and soft copies of the assessment forms will be saved in the secure Data Store SharePoint Folder dedicated to this research study. All electronic data will be treated with strict confidentiality and will only be accessible to the Principal Investigator and Co-investigators. Data monitoring and audits will be conducted by the SIT Institutional Review Board.
The research data will be retained for governance purposes and destroyed after ten years upon completion and publication of the research findings.
Sample size calculation and statistical analysesThe randomized controlled trial by Katsumi and colleagues [59] is used to provide the effect size of NEAR versus control arm receiving standard psychiatric rehabilitation. Functional outcome of this study is measured using the Global Assessment of Functioning (GAF). The mean GAF scores of both arms at the first follow-up post-intervention are used in this sample size calculation. Using G*Power 3.1.9.7 calculator [60], with cohen’s d = 0.48, α = 5% and β = 85% on a two-tailed test, the number of participants required at each arm is 79. To round off, 80 participants will be needed at each arm, making the total number of participants in our study to be 160.
Stata18 statistical package [61] will be used to present the demographic profile, calculate the descriptive statistics and to analyze the data. Intent-to-treat analyses will be carried out, hence one-to-one replacement for participants who drop out will not be carried out.
First, a comparison of the demographic characteristics and baseline outcome measurement scores of the participants in both arms will be carried out, to delineate any significant differences. Second, Repeated Measures ANOVA will be carried out to test for group by time differences in neurocognition and social cognition performance (measured by BACS and BLERT), symptoms (measured by PANSS and BNSS), functioning and recovery (measured by SOFAS and COPM), metacognition (measured by WCPA) and metamotivation (measured by BroMS) across the three time points of baseline, post-intervention and eight-week follow-up.
Next, regression analyses will be carried out with SOFAS and COPM separately as dependent variables, to determine factors which may predict functioning and recovery. Correlation analyses will also be conducted to test for associations among neurocognition, social cognition, negative symptoms, metacognition, metamotivation, functioning and recovery. Lastly, bootstrapping will be carried out to test for mediators for improvement in cognitive performance and functioning.
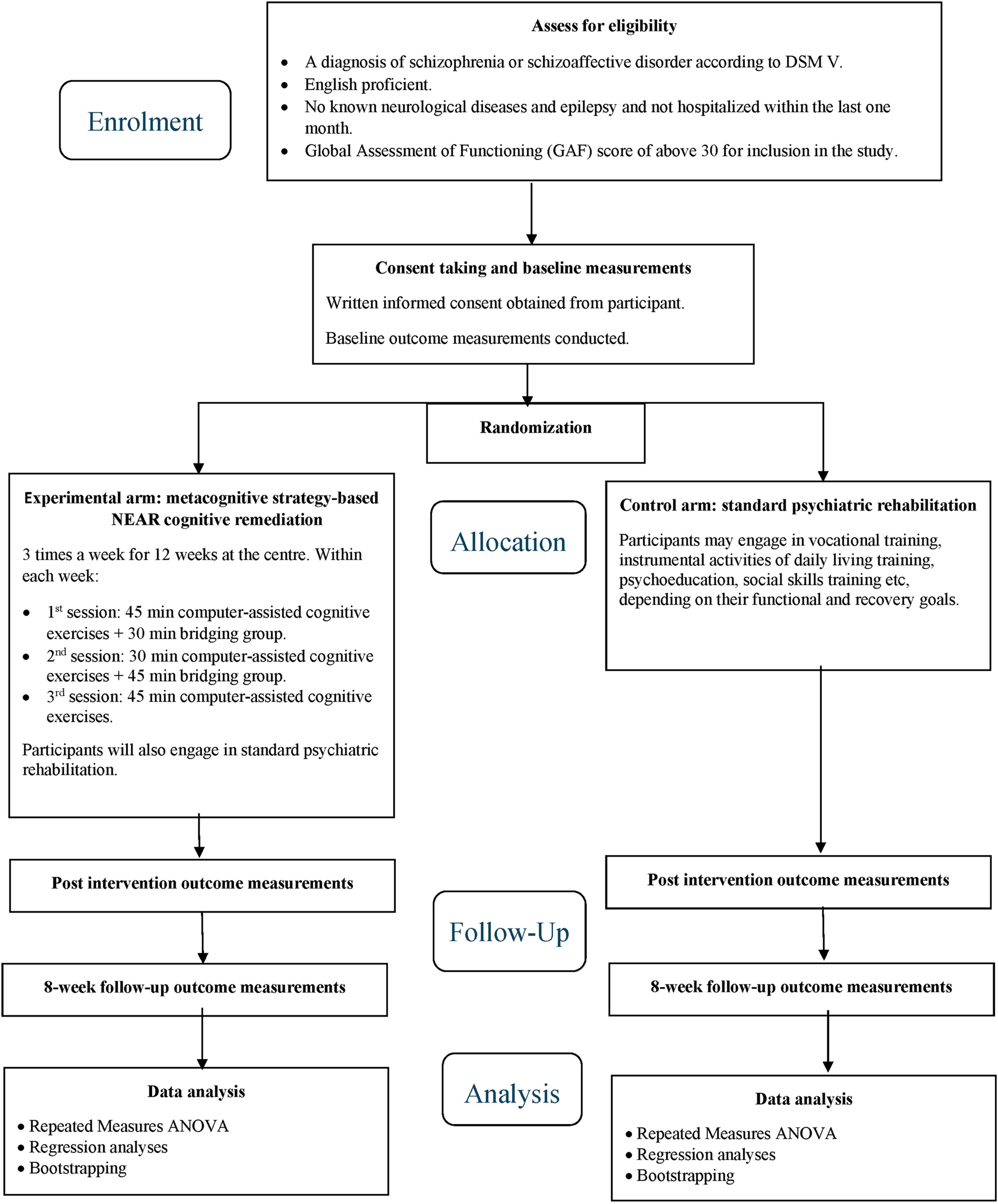
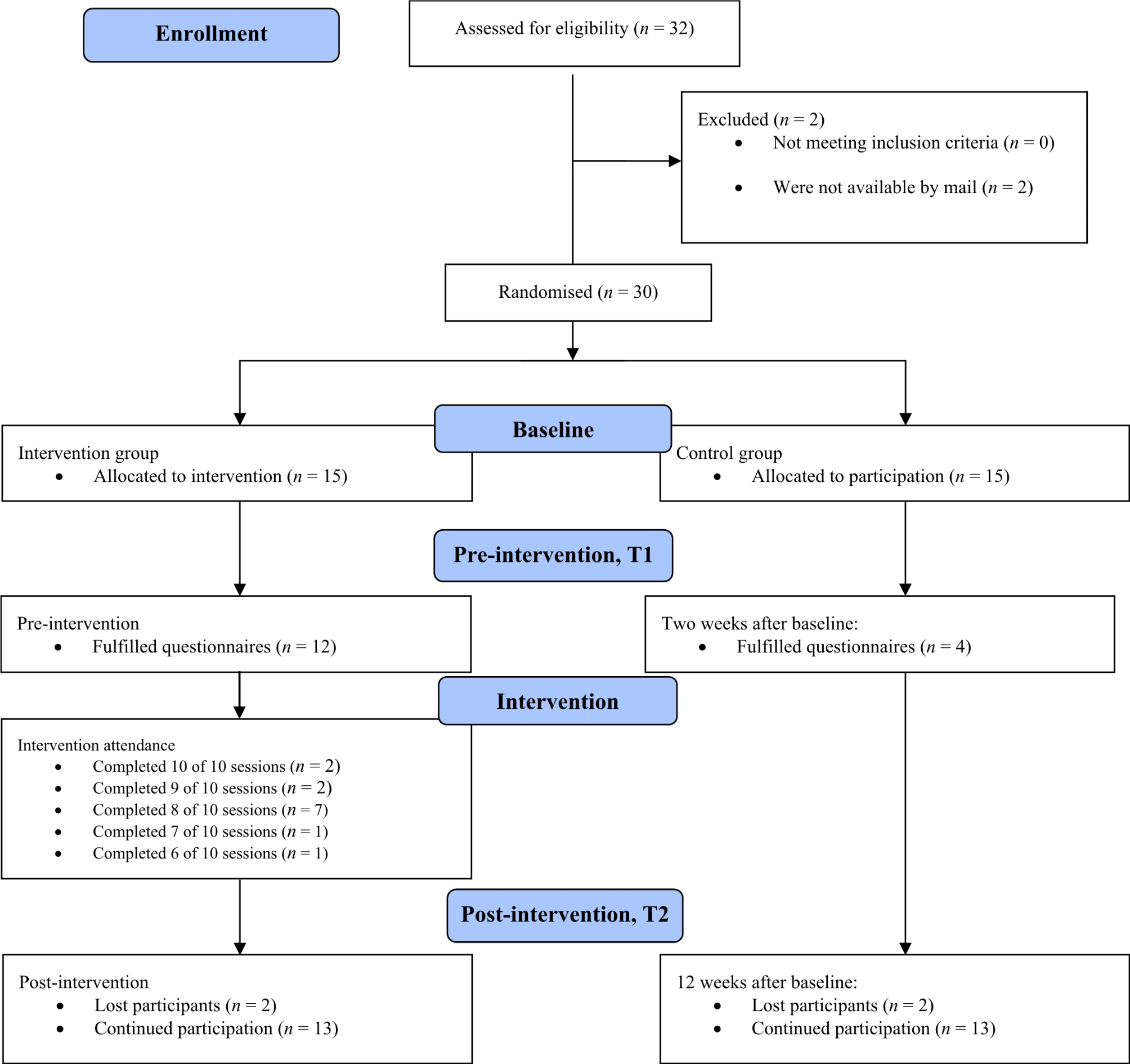
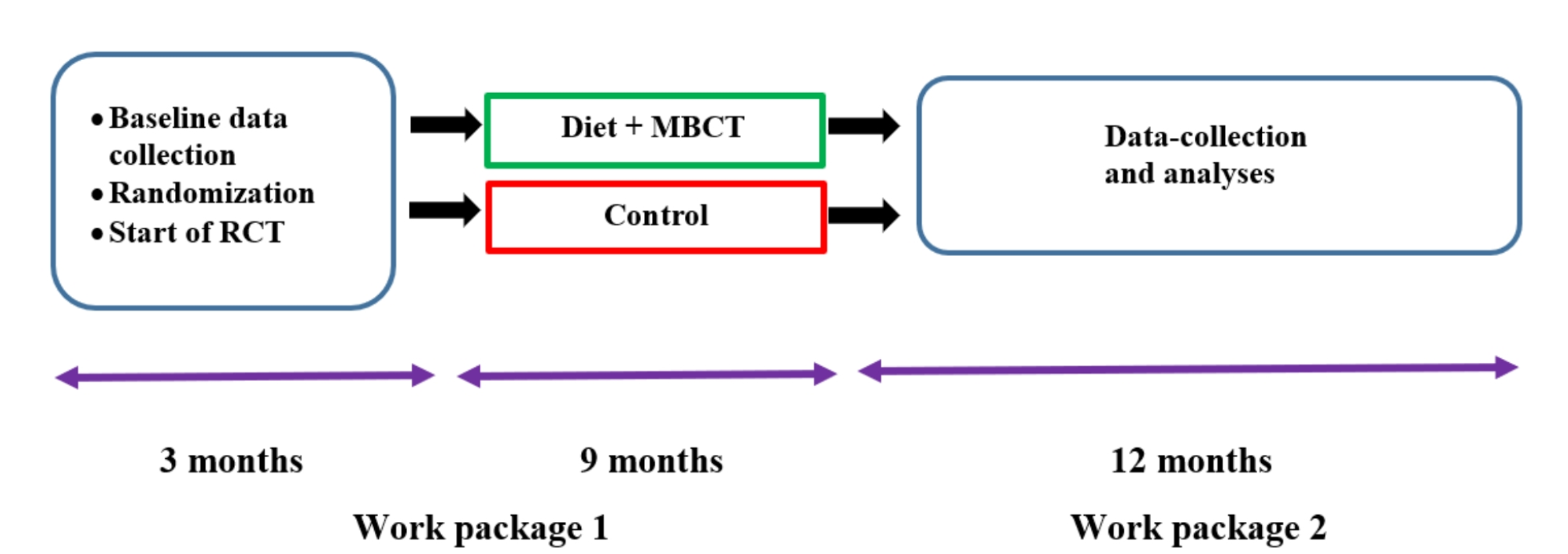
See Fig. 1 for the flow diagram of the study procedure.
Fig. 1
留言 (0)