The hemodynamic impact and the morphology of LVOT-obstruction in HOCM-patients is of ongoing interest and remains a challenge. In our analysis of LVOT obstructions in HOCM three main types could be identified. These shapes were characterized by different hemodynamic patterns with the V-shape displaying the most pronounced obstruction. To the best of our knowledge this is the first study describing different LVOT-obstruction shapes using a CMR based 3D reconstruction approach.
The septal hypertrophy described in all three obstructive shapes led to a unanimous unilateral reduction of volume while the bilateral obstructive narrowing was induced by different structures such as the anterior leaflet of the mitral valve or the papillary muscles. The K-shape was based solely on septal hypertrophy. The X- and V-shapes showed similarities in their formed anatomies in the septal hypertrophy and the SAM-phenomenon, however the V-shape’s distinctive influence was caused by an asymmetric thickness and the hypertrophy of the papillary muscles. This further underlines the impact of the papillary muscle size [16, 17]. In HCM the quantification of the papillary muscles as a part of the myocardium are impactful, as they influence the stroke volume as well as the obstruction. Another shape was the so-called mixed shape. This is neither a new main shape nor a shape that can be directly categorized, as it changes its external appearance during the systolic phases. Different aspects of the three main categories were all present within in this shape. Anatomically, the same features of the other categories are also present, which result in an obstructive pattern. It is speculated that this might be an intermediate form in the progression of the disease. However, we cannot confirm this precisely, as the number of patients with this type was the smallest within the cohort. On the other hand, patients who had multiple scans over several years showed consistency in the assigned category after the initial measurement. Therefore, it remains questionable how the mixed shape should be evaluated. Further analyses with new measurements would be necessary for this.
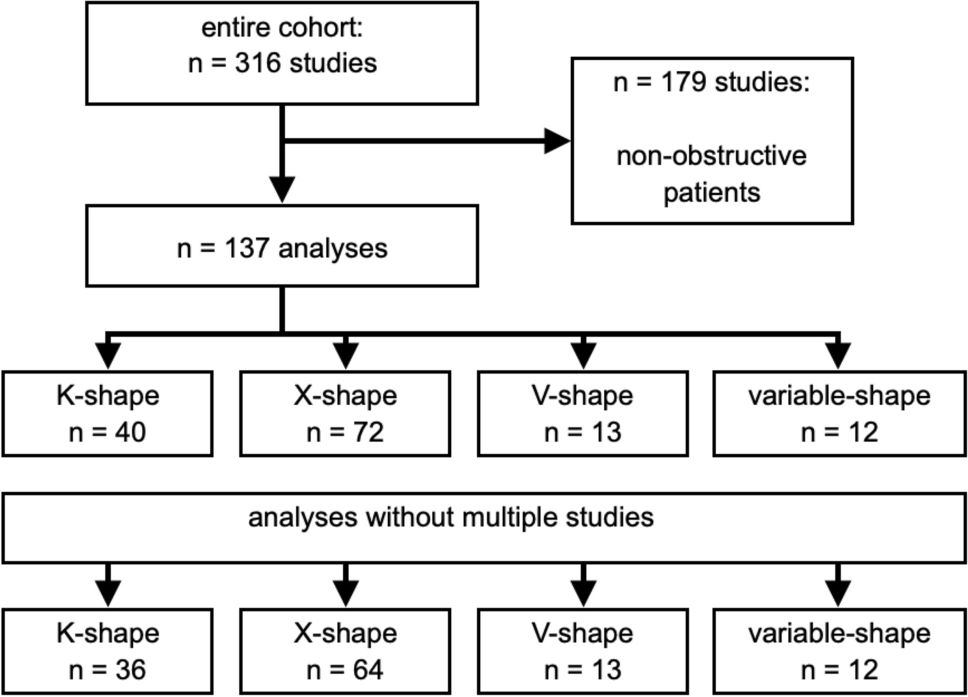
In the NHLBI HCM Registry (HCMR trial) different phenotypes of HCM could be identified. With such a vast prospective cohort, the asymmetric septal hypertrophy was shown to be the most common phenotype [4]. In our analysis of the distribution (Fig. 4), it was evident that the K- and X-shape are the most common shape of obstruction. These primarily result from a local hypertrophy of the septum, which aligns with the finding that septal hypertrophy is the most frequently occurring. This leads to a direct local impact on the LVOT-pathway and thus to altered flow patterns in the sense of an obstruction. Usually, the pressure gradient is used to quantify the obstruction. Techniques like 4D Flow CMR may provide additional information, but they are not currently applied in clinical routine in CMR despite the application in congenital heart disease. 4D Flow CMR visualization is widely used in such patients as advised in the guidelines [18]. In HCM Allen et al. [2] could show that different grades of obstructive flow profiles could be differentiated by velocity isosurfaces of the LVOT using 4D Flow CMR imaging. They have pointed out the relevance of the SAM-phenomenon by identifying a pronounced helical flow in patients with obstruction. Based on our in-vitro experiments we hypothesize that helical flow patterns causes the flow phenomenon. Our phantom provides information at the time of end-systole, which is the point of maximum obstruction. It is known that helical flow patterns increase with the severity of the obstruction. To create identical conditions among our obstruction shapes, we normalized the area of narrowing in all three phantoms. It was found that despite the identical conditions, flow patterns were different, and the intensity of the helical flow varied among the shapes. Care was taken to identify the one with the most significant obstruction. The LVOT could be compared with a nozzle inducing a jet flow [24]. These jet formations represented the three main obstructive shapes. Interestingly, even the X- and V-shapes, although very similar in shape pattern, showed different flow profiles. We can only assume that the higher velocity in the V-shape was induced by the steeper nozzle shape. However, we can also see that although the V-shape has the highest flow acceleration, it does not have the strongest manifestation of helical flows. This is actually seen in the K-form. Thus, it becomes evident that not only the diameter of the narrowest point but also its position within the LVOT has an impact. However, obstruction in HCM is also related to heart rate and loading conditions [1, 9], therefore a flexible phantom could further add knowledge in this matter of interest. The properties of the mixed shape would also need to be measured in a dynamic phantom or in-vivo.
In the past, the LVOT area was assessed using not only CMR but also by 3D echocardiography [9]. It is known that the assessment of LVOT obstruction based on pressure gradient depends on loading conditions leading to fluctuations [2, 3, 6]. CMR combines the advantages of non-invasive and invasive methods. MRI diagnostics are widely used and less dependent on the examiner compared to echocardiography. Non-invasive flow analyses can also be performed, for example, to evaluate obstructions without relying on the fluctuations and indirect determination of the pressure gradient as in echocardiography or the invasive approach of cardiac catheterization. Therefore, CMR is a suitable method for diagnosis and monitoring in patients of all ages. Using our current 3D approach based on time resolved cine-images information about the lengths and shape of the LVOT obstruction could now be added as a control factor. However, there are also notable limitations in reconstructing 3D volumes from 2D slices. The need to hold one’s breath and take successive measurements can lead to shifts between the slices. This is a known issue, but it is tolerated in clinical settings. It is standard practice to analyze functional cardiac parameters from 2D slices [19]. To minimize this phenomenon in our reconstructions of the LVOT (left ventricular outflow tract), multiple checks were performed using anatomical landmarks. When the reconstructed LVOT is viewed in a three-chamber view, there is good alignment of the contours with the anatomical images. It is also worth mentioning that far fewer slices are required for LVOT reconstructions compared to a complete coverage of the entire left ventricle. Thus, a single breath-hold is usually sufficient. Another point to note is that we observed that patients with multiple measurements at different time points (follow-up) showed no changes warranting a different categorization. Nonetheless, expanding the concept to include 3D cine technique would be beneficial. However, this technique is not yet standardized and involves additional components that need to be considered. For instance, the blood-myocardium contrast can be limited without special attention to contrast agent administration, making in-vivo measurements more cumbersome, and insufficient attention to this aspect can complicate the evaluation of LVOT components. Additionally, alignment software is needed, which is still under research. The aforementioned artifacts from breath-holding would be reduced, and trials have shown that measurement times could be decreased [20]. In summary, our current understanding is based on clinical standard measurements and established evaluation techniques, but it is certainly advisable to conduct further analyses using newer measurement methods.
We believe that detailed information about each specific phenotype of obstruction is warranted due to different interventional and surgical therapeutic options being available in patients with HOCM [1]. The interventional approach TASH (transcoronary ablation of septal hypertrophy) depends highly on the anatomy of the septal arteries [1]. The decision making is complex and is primarily based on the localization and type of hypertrophy. The obstruction can also be influenced by the morphology of the mitral valve. There are numerous variations such as longer leaflets or abnormalities in the mitral apparatus [8] guiding the decision towards myectomy. A 3D-model driven surgery is well-known already in other fields of cardiology and cardiothoracic surgery e.g. congenital heart disease [21, 22].






留言 (0)