
記住我
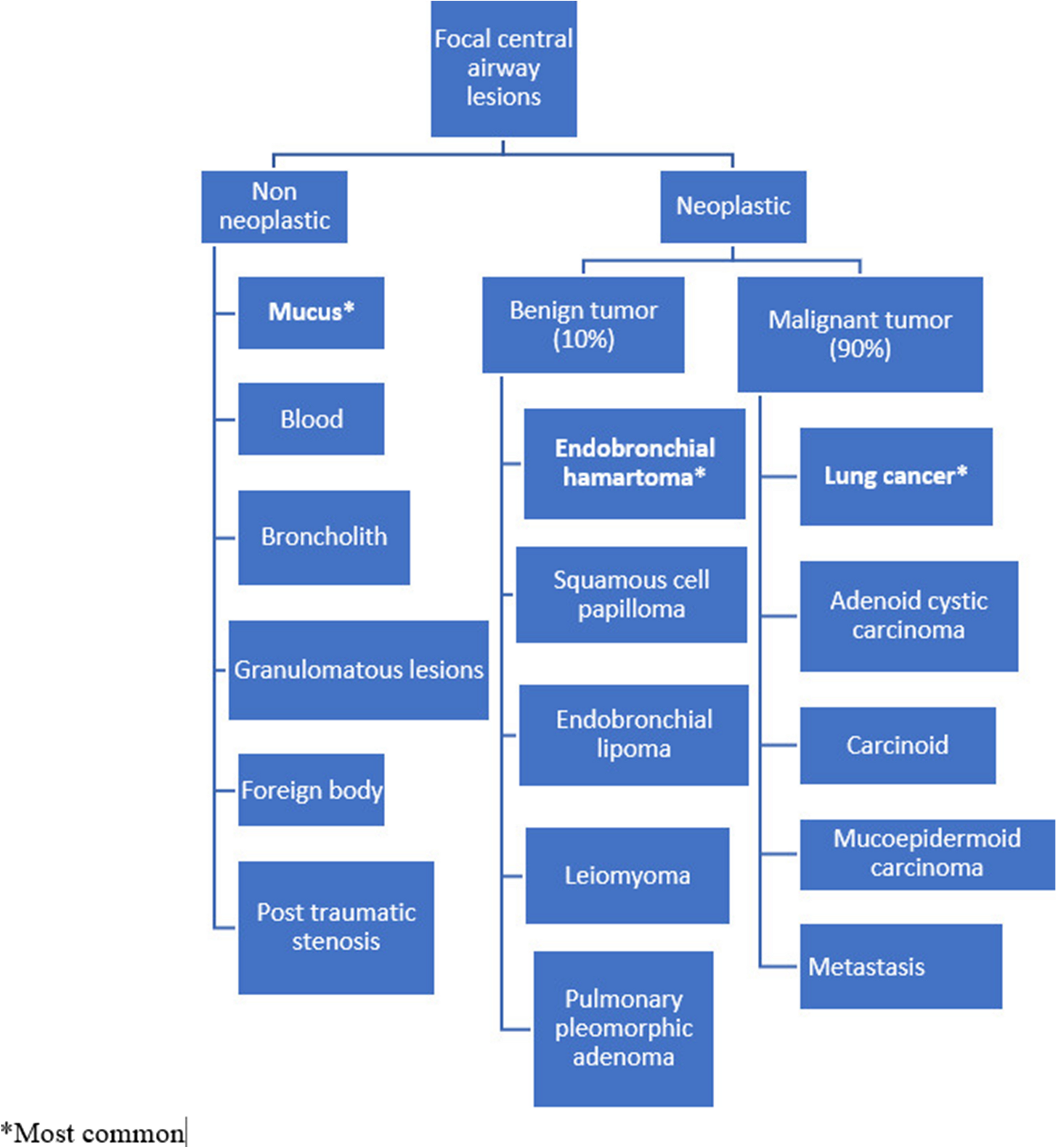

A 60-year-old male with a known history of hypertension experienced redness, blurred vision, and severe pain radiating to his head. He underwent cataract surgery at a local hospital, but symptoms persisted, leading him to a higher centre.
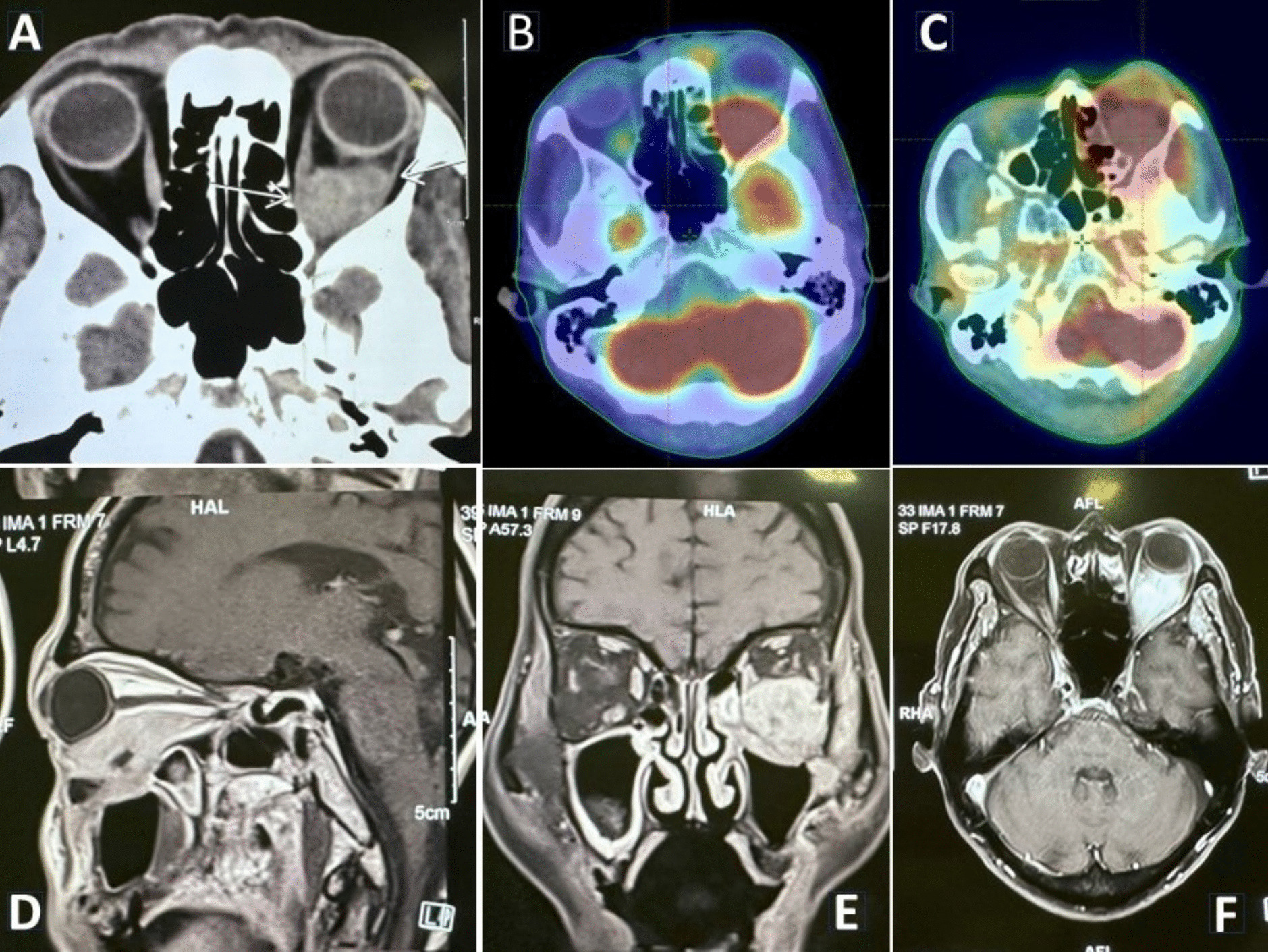
Contrast-enhanced magnetic resonance imaging (CEMRI) of the orbit revealed a large irregular lesion (60 × 52 × 31 mm) in his left orbit predominately in the inferior part, involving inferior rectus muscle in its entirety up to orbital apex and extension infero-laterally through superior orbital fissure into left infra-temporal fossa, masticator space, left maxillary sinus with bony dehiscence in the posterior wall of left maxillary antrum, inferior aspect of lateral orbital wall. The left pterygoid muscle also involved. The cavernous sinus was spared and no intracranial extension was seen (Fig. 1). Biopsy confirmed squamous cell carcinoma of the orbital wall (Fig. 2). Following this, the patient was referred to us for further management.
Fig. 1
Pre-treatment images. a Axial CT; b, c axial PET-CT; d CEMRI sagittal, e CEMRI coronal, and f CEMRI axial showing an irregular mass lesion in the left orbit in retroorbital space predominately in the inferior part
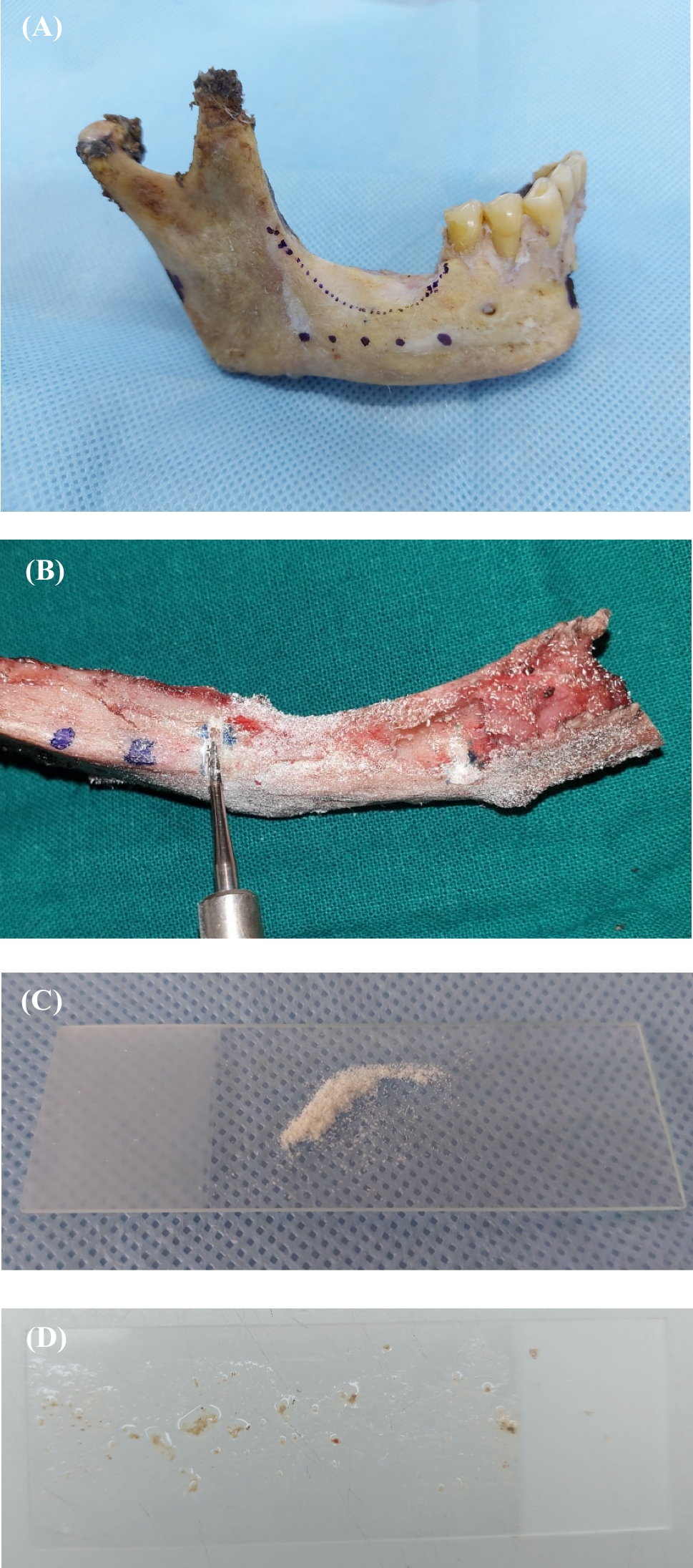
Fig. 2
HPE showing fibromuscular tissue infiltrated by squamous cell carcinoma, moderately differentiated
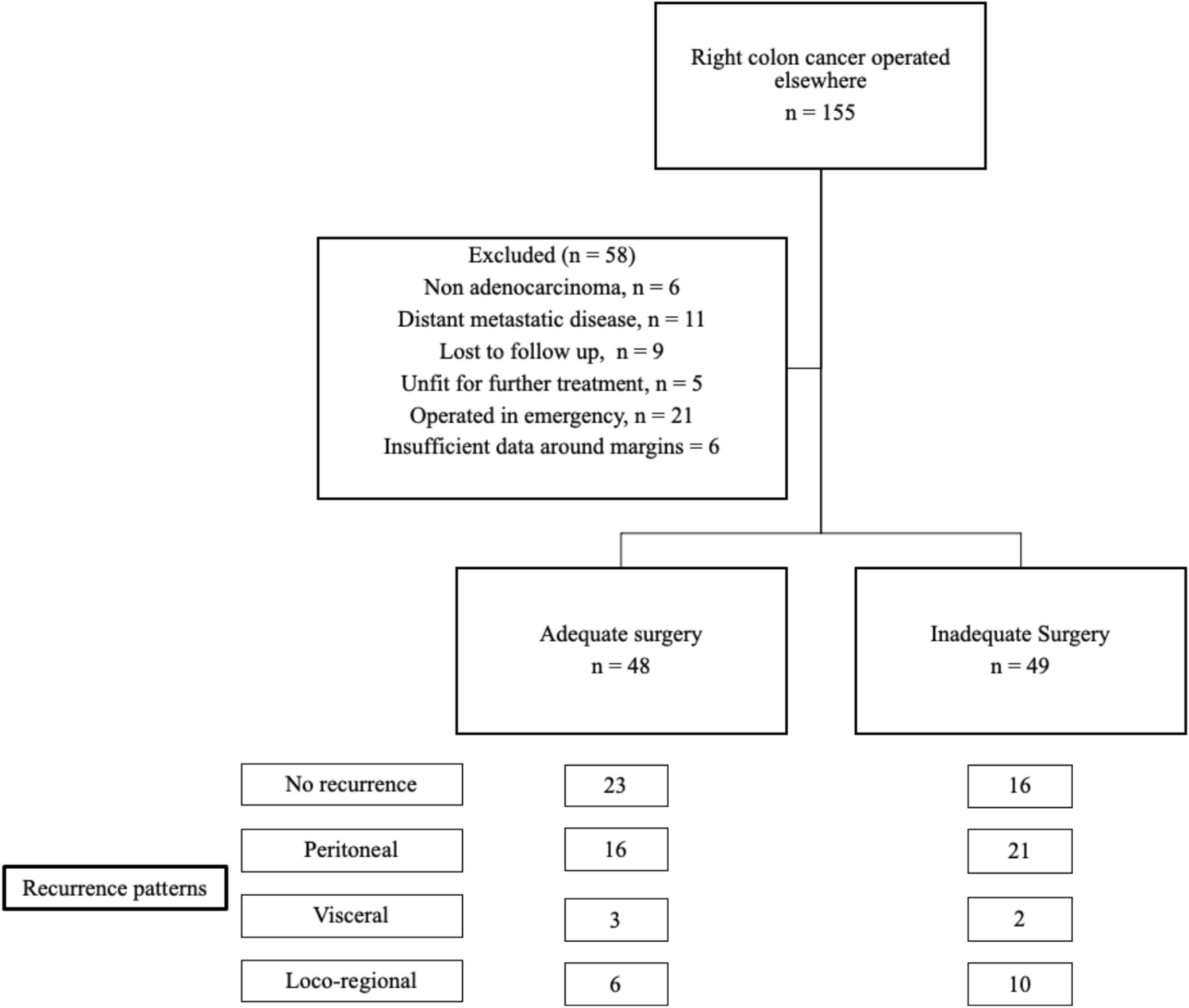
At that time, the patient also developed diffuse swelling over the right eye (Fig. 3A) and right side of the face along with the existing symptoms. PET-CT was done which showed 3.7 × 3.4 × 4.5 cm mass in the left retrobulbar region, left maxillary sinus extending to the infra-temporal fossa (ITF) (SUV max11.9) (Fig. 1). No evidence of distant metastasis was seen.
Fig. 3
Clinical image of the patient: a pre-treatment image showing swelling and redness of the left eye; b 15 months post-treatment showing good clinical response
The case was then discussed in an institutional multidisciplinary tumour board. Surgical opinion was taken and he was deemed inoperable as R0 resection was found not feasible. He was then planned for definitive radiotherapy with concurrent chemotherapy.
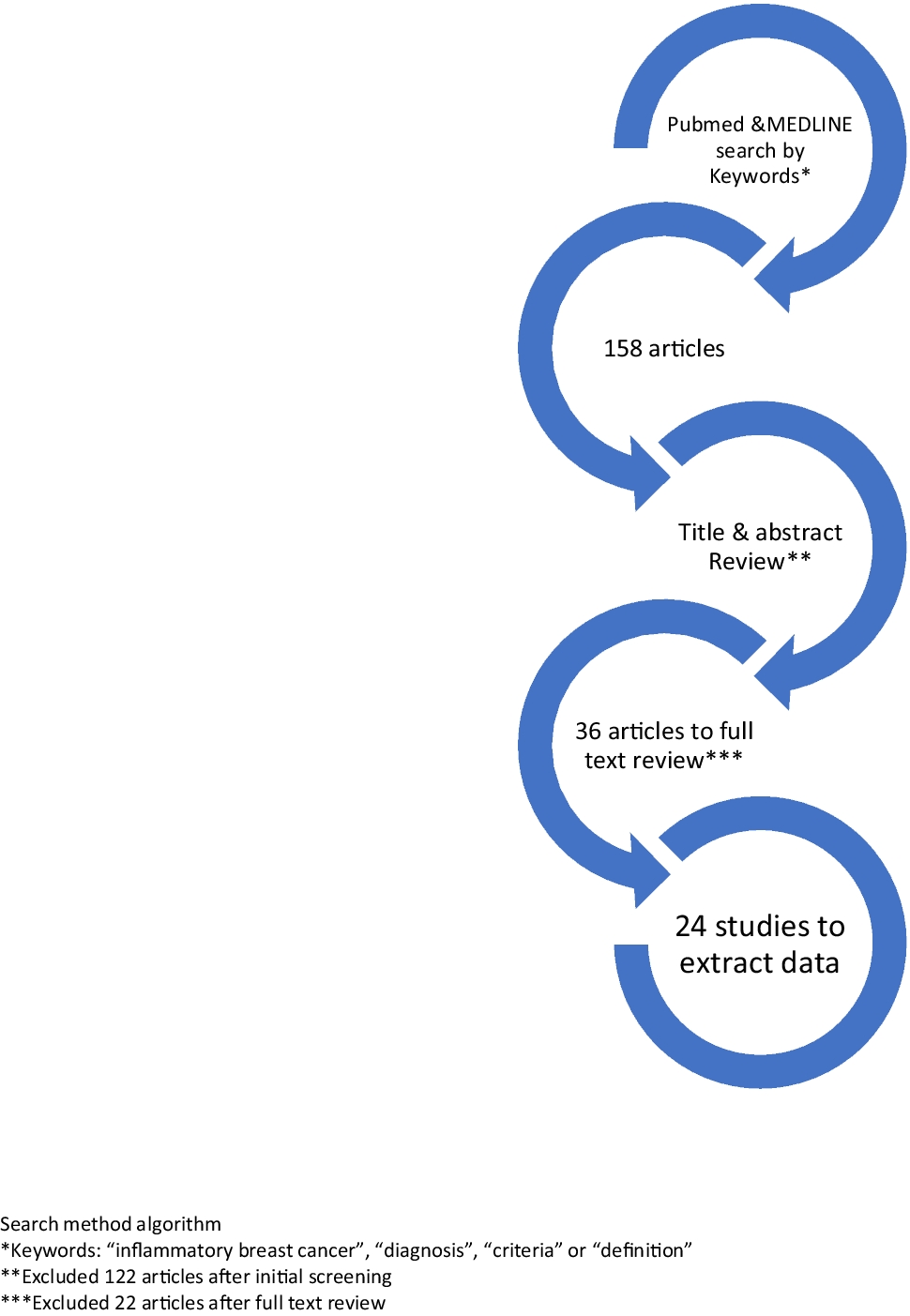
Radiotherapy: The patient was treated with external beam radiotherapy (EBRT) to a dose of 60 Gy in 30 fractions from 5/1/23 to 25/2/23 using VMAT technique (Fig. 4).
Fig. 4
Axial dose wash of volumetric modulated arc radiotherapy treatment plan
The patient was immobilised in the supine position using three clamp thermoplastic brain mold. Intra-venous contrast-enhanced CT images were acquired after ensuring normal renal function (serum creatinine level and creatinine clearance) using the PhilipsCT simulator with 3-mm slice spacing. In digital imaging and communication (DICOM) format, these simulation images were exported to the Varian Eclipse treatment planning system (TPS). The patient’s MRI and PET-CT images were fused with the planning CT images. The gross tumour volume (GTVp) was delineated with aid of these images. A high-risk CTV was created to include areas of microscopic tumour involvement with a margin over the GTV by 10 mm, excluding the regions of air or bone without evidence of tumour invasion. The planning target volume (PTV) was created by adding a 5-mm geometric expansion over CTV. Organs at risk (OARs) were contoured as per institutional protocol.
Dose prescription was 60 Gy in 30 fractions to in PTV. The planning objectives for PTV were set such that 95% of PTV volume should receive at least 95% of the prescribed dose. The maximum dose (V107%) was restricted to less than 1% volume of PTV.
Normal tissue tolerance of radiation dose was respected as per the Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) data. Dose-volume parameters for OARs are set as the maximum dose (Dmax) of the spinal cord (< 45 Gy), brainstem (< 54 Gy), optic chiasm (< 54 Gy), optic nerves (< 54 Gy), eyeball (< 45 Gy), and lens (< 10 Gy), and (Dmean) for parotids, cochlea (< 45 Gy), etc.
VMAT planning was done using the Eclipse TPS. VMAT plan was delivered with 6-MV X-ray beams with Varian Trilogy linear accelerator. Treatment setup verification was done with CT image guidance. The protocol of image guidance was daily for initial 3 days and then twice in a week. Radiotherapy was delivered five fractions in a week.
Chemotherapy: 6 cycles of weekly concurrent chemotherapy with 60 mg cisplatin @40 mg/m2 was delivered during RT.
Follow‐up and assessment: The patient was clinically assessed weekly during the treatment period. The patient tolerated the treatment well. At conclusion, the patient had acuity of vision within normal limits. After completion of treatment, the patient was subsequently followed up every 2 months by means of complete physical examination and imaging. The patient experienced occasional eye pain but maintained normal vision during follow-up visits.
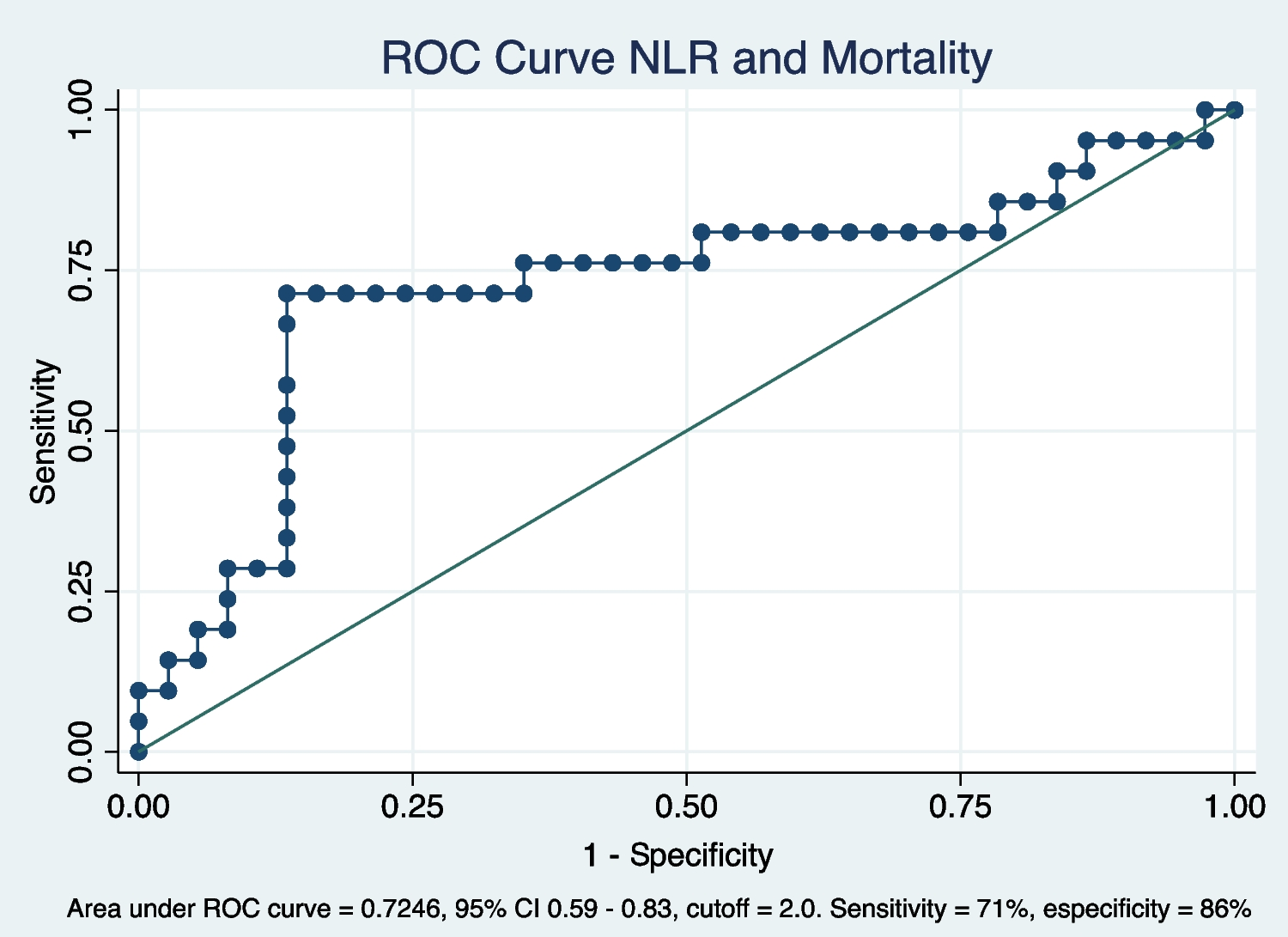
At the first follow-up after 2 months of completion of RT, an MRI was done which showed residual lesion measuring 24 × 28 × 19 mm in size in the retrobulbar space of the left orbit in its inferior aspect involving both intraconal and extraconal regions along with post-treatment changes. The patient then came for second follow-up after 3 months; he had normal vision and no fresh complaints back then. A whole-body PET-CT scan was advised at 6 months of treatment completion. Compared to previous scans, the PET-CT scan showed a complete metabolic response (Fig. 5).
Fig. 5
PET-CT images comparing pre-treatment and post-treatment. a Pre-treatment images showing the disease; b 6-month post RT showing complete resolution of the disease
The patient continued routine follow-up appointments, with complete clinical and radiological response till last follow-up which was 15 months post radiotherapy (Fig. 3B). Ophthalmology consultation was advised for cataract screening and power adjustment, with regular follow-ups scheduled in the radiation oncology department.
留言 (0)