This study aimed to culturally adapt MHFA guidelines for EDs in Iran using the Delphi expert consensus method. The participants included health professionals and individuals with lived experience of EDs.
Agreed recommendations
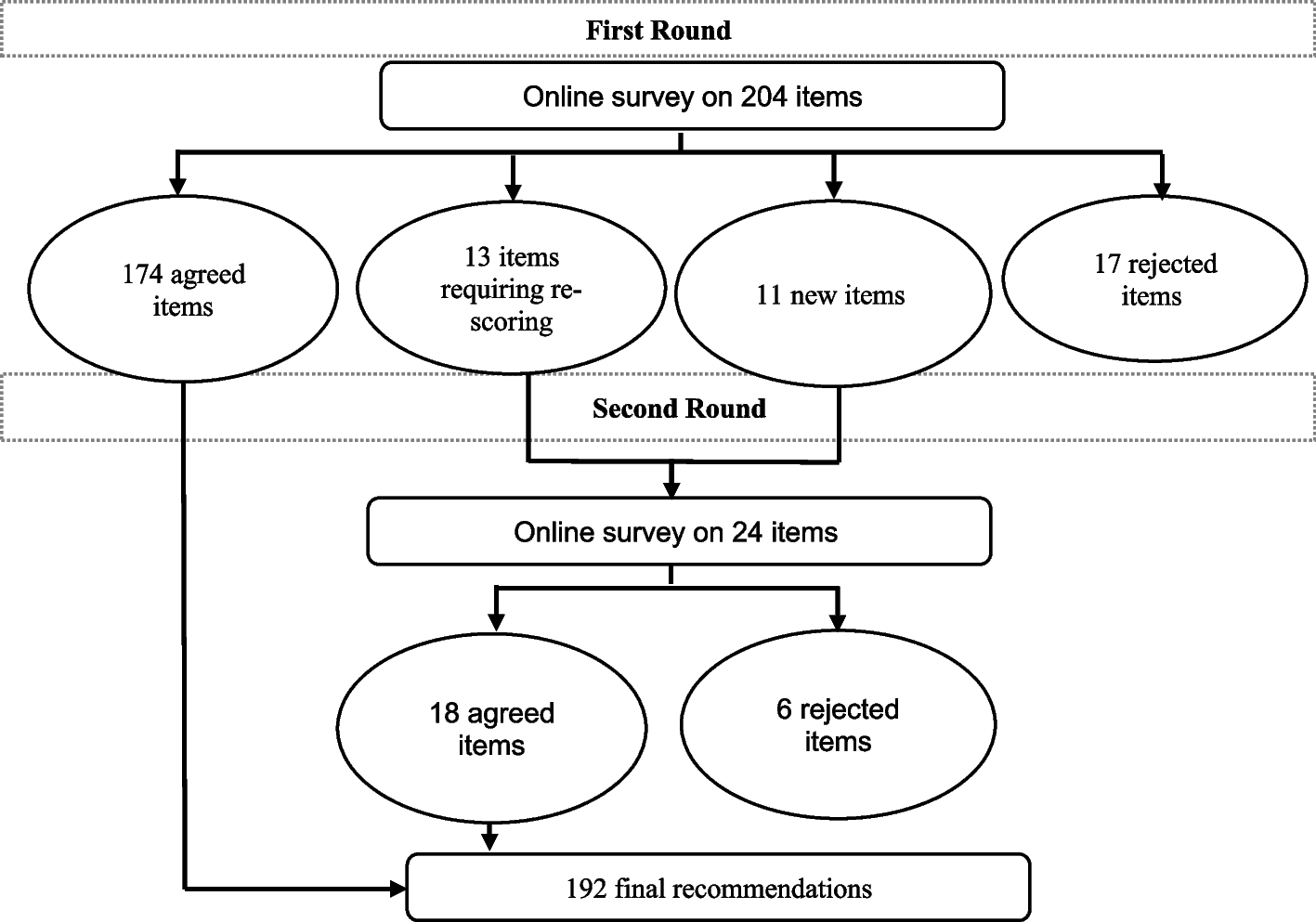
Over 90% of the items in the English-language guidelines and seven of the 11 newly suggested items by the panel were endorsed. Most of these items (85.3%) were confirmed in the first Delphi round, with only 5% added in the second round. Previous studies have shown that the MHFA guidelines series has strong scientific support, suggesting that accepting and implementing these guidelines' recommendations will encourage Iran to adopt an evidence-based approach to EDs interventions. As Jorm previously noted, a high number of approved recommendations in a country indicates the high generalizability of the reference guideline. When there are social similarities between countries, the likelihood of accepting many guideline recommendations increases in the destination country [51]. Guidelines' recommendations should be adapted to the country's socioeconomic and cultural circumstances. For example, in a study about implementing MHFA guidelines in the deprived region of Uganda, Hays found challenges in health service infrastructure and a lack of cultural compatibility [52].
A comparison of the number of approved recommendations across the eleven areas showed that understanding EDs and recognizing their warning signs were the most critical. In line with the present study, Hart's study found that the area of understanding and awareness had the highest number of accepted recommendations (60 cases) [47]. According to Mond, a key factor explaining low health literacy about EDs is that some of these disorders, like binge eating, have only recently been recognized as psychiatric disorders. There is also low community awareness of EDs due to widespread beliefs that they are not prevalent or severe, stigma towards those affected, and demographics such as gender concerning MHL related to EDs [53].
However, researchers have paid less attention to Iranians' health literacy regarding EDs. Studies on the country's population have mainly focused on food and nutritional literacy (knowledge, skills, and behaviors related to a healthy diet and adherence to it) [54, 55]. In line with one of these few studies, only about 11% of Iranian youths had good health literacy about EDs, and about 34% were not confident in their ability. This cross-sectional study was performed on people aged 16–29 living in Tehran to measure health literacy about EDs. This study emphasized the importance of friends and family in supporting people with EDs, providing MHFA in simple language, educating those affected on how to manage their condition, and informing them about the professional services and help available [56].
Rejected recommendations
In this study, the most frequently deleted recommendations, with a total of four items, pertained to the areas "How to approach someone with EDs?" and "How to express concern to the affected person?" The central idea behind these areas is effective communication with individuals in need. According to research findings on MHFA guidelines for assisting people with alcohol abuse in Chile and Argentina, the guidelines should align with the cultural orientation of the destination country to respect the wishes and expectations of the person needing help regarding interpersonal relationships [39]. Consequently, Fernando et al. identified linguistic respect for autonomy and the right to refuse professional help as reasons for omitting several recommendations from their panel in a study on MHFA aid for depression in Sri Lanka [40].
Additionally, countries may have different service delivery models, risk factors, and vulnerable populations [57]. Studies have shown that the prevalence of EDs in Iran, similar to other developing countries, is influenced by a combination of cultural, socioeconomic, racial, and genetic factors [5]. Another study highlighted that cultural issues, such as religion and the practice of wearing a hijab, are significant socio-cultural factors to consider when analyzing EDs in Iranian populations [6]. The eating behaviors of the Iranian population in the southern regions are shaped by factors such as access to food, food preferences, cultural values, family beliefs, and practices related to cooking and storing food [58].
Moreover, evidence suggests that Iranian women and children are particularly vulnerable groups that require special attention [6, 7]. Therefore, addressing these groups' unique emotional and communication needs is essential when preparing MHFA guidelines. In the present study, various Iranian cultural characteristics, including stigma towards mental health disorders, religious beliefs and rituals such as fasting, linguistic differences between English and Farsi, the influential role of family and friends, trust in others, and ethnic diversity were considered in rejecting and rewriting recommendations.
New recommendations
As mentioned earlier, in the Iranian adaptation, seven out of the 11 new recommendations were confirmed and incorporated into the final guideline. These new recommendations fall under two main areas: "How to deal with the affected person" and "The role of a young first aider in helping a friend suspected of having an EDs.".
Regarding the first new recommendation, "The first aider should be aware that the nutritional customs can differ in every region of the country," it is important to note that Iran's vast geographical and ethnic diversity results in distinct regional food cultures. Participants emphasized that first aiders should consider these cultural customs when addressing dietary restrictions related to food type and quantity rather than solely focusing on EDs. A 2023 review highlighted the importance of considering variables such as ethnicity when estimating and determining the prevalence and risk factors of EDs, consistent with the current study [59]. Another study emphasized the role of values and beliefs, identifying factors such as maternal education, attitudes and practices regarding children's nutritional habits, socioeconomic status, country of residence, culture, ethnicity, religion, and superstitions as determinants [60]. Furthermore, the versatility of diets among Iranians and their association with the emergence of disorders has been confirmed [61]. Another study identified several influential factors in Iranian dietary preferences, including family traditions, experiences, values and beliefs, societal and cultural factors, interest in traditional medicine, life priorities, access to resources, cooking skills, and religious beliefs [62].
The second and third recommendations, "The first aider must try to earn the person's trust" and "The first aider should not treat the person as if they are helpless," address the significant stigma associated with psychiatric disorders, including EDs, within Iranian culture. This stigma can lead to social isolation or ridicule for individuals with EDs. Participants endorsed these recommendations to raise awareness among first aiders and prevent behaviors that contribute to these negative outcomes. Supporting this finding, a cross-sectional study reported that stigma is one of the main obstacles to seeking professional help among Iranian women struggling with obesity, highlighting the importance of considering stigma in the design and implementation of interventions [63].
The fourth recommendation, "The first aider should use simple language," highlights the participants' emphasis on the importance of avoiding scientific expressions and terminology when interacting with and assisting individuals suspected of having an ED. This recommendation addresses the issue that trained individuals may often use jargon, which can harm the first-aider-patient relationship. The importance of practical training on how to appropriately communicate with individuals with mental health disorders has been emphasized in several studies [64]. For instance, effective communication with affected individuals was a critical factor considered in Li et al.'s study for developing MHFA guidelines for alcohol problems [38].
The fifth recommendation, "The first aider should direct their feedback to future actions and try to motivate the person," reflects the participants' experiences in motivating individuals. This recommendation was added to the guidelines to emphasize the importance of motivation in aiding individuals with EDs. Several studies have highlighted the role of motivation in the recovery of patients with EDs, noting that long-term motivation can promote treatment adherence and reduce susceptibility to false social values and norms [65, 66].
The sixth recommendation, "The first aider should consider the influence of peers when thinking about how to help the person," was added to the guideline in recognition of the strong influence peer groups have on each other. This recommendation encourages first aiders to leverage peer groups to support adolescents showing symptoms of EDs. In research conducted to adapt MHFA for suicide in China, Lu et al. emphasized the importance of considering factors such as the community's attitude towards suicide and the role of families and friends [48, 49].
Several studies have emphasized the necessity of considering the role of peers when designing administrative and preventative eating disorder interventions [67, 68]. Peers can significantly support adolescents with EDs. By training select individuals, health ambassadors can be empowered to use peer influence to educate others about unhealthy eating habits. When considering the role and effectiveness of these trained individuals, it is essential to account for gender differences [69].
The seventh and final recommendation, "The first aider should try to separate their friendship and first aider roles when helping the person," emphasizes the importance of adopting a specific approach to overcome barriers when supporting a friend with symptoms of an EDs. This approach allows first-aiders to balance their roles as friends and caregivers. By establishing a distinct time and communication framework, first aiders can offer essential support during critical moments while preserving the core of their friendship. Once the immediate crisis is resolved, the friendship can resume. This recommendation stresses the need for clear boundaries and a structured method for providing support, ensuring the effectiveness of aid while maintaining the dynamics of the friendship. By separating these roles, first aiders can minimize conflicts of interest, uphold the individual's autonomy, and address ethical considerations such as confidentiality.
Recommendations with more than 10% difference between the two panels
Another notable finding of the study was the significant number of recommendations with more than a 10% difference in the percentage of agreement between the two panels of health professionals and individuals with lived experience. Similar to our study, McMaster et al. confirmed the differences in views on EDs among health professionals, consumers, and caregivers [70]. In Hart et al.'s study, 13 recommendations showed a significant difference of opinion between the panels, attributed to differences in attitudes towards preserving patient privacy, recognizing and acting on emergencies, and respecting patient autonomy versus making decisions for the patient [47].
Additionally, another study assessed the differing educational needs of the general population and specialists, including general practitioners, psychiatrists, gynecologists, gastroenterologists, medical students, paramedics, managers, teachers, coaches, and gym workers. This study suggested employing various strategies to enhance these groups' ability to recognize EDs. Recommendations included improving the initial training process and its continuity, emphasizing electronic platforms for specialists, enhancing MHL, and implementing MHFA training programs for the general population [71].
The significant difference in opinions on many items is likely due to the varying levels of awareness and knowledge between the two groups about the signs and symptoms of EDs, coping strategies, the need for professional help, and the necessity and importance of first aid. This highlights the critical need to provide education and increase awareness at the community level.
The item "hiding their behaviors from their family and loved ones, the first aider should tell a responsible and trusted adult, even if it is against the friend's wishes," highlights the community's strong emphasis on maintaining friendship, loyalty, trust, and confidentiality. Evidence indicates that respecting the rights of patients with EDs and acknowledging their autonomy in decision-making is essential for enhancing their engagement and adherence to treatment [72].
Regarding the items "The first aider should be aware that there is no quick and easy solution to overcoming an eating disorder, but effective treatment is available" and "A person with EDs will benefit from professional help," the discrepancy between the two groups may stem from differing perceptions. People with lived experience might hold misconceptions about EDs, such as believing that willpower or simple lifestyle changes can overcome them. This could explain the lack of agreement, as there may be a lack of understanding of the severity and complexity of these conditions. Conversely, health professionals possess in-depth knowledge and experience working with individuals with EDs. They understand the challenges in treating these conditions and are more likely to recognize the necessity of professional help and the absence of quick fixes.
For the item "If the child becomes harmful to themselves or others, the parent must be prepared to move them to a safe environment, such as a hospital," the agreement rate from the community group was below 70%. This may be due to societal stigma and misconceptions surrounding mental health issues, leading to reluctance to acknowledge the severity of the situation and the need for immediate professional intervention, such as hospitalization. Further research is needed to understand the factors influencing parents' reluctance to hospitalize their children for psychological disorders.
Strengths and limitations
The participation rate in the first round of the Delphi study was 57.6%, possibly due to the large number of items examined (204 items). In the second round, a participation rate of 80% was achieved, with only 24 items discussed. The high participation rate in the second round may be attributed to the participant's familiarity with the study, as the questionnaire link was sent only to those who participated in the first round.Other limitations of this study include the similarity of specialized topic-related guidelines and the lack of valid evidence for comparing and interpreting the results. To address this, a widely-used guideline with proven efficiency in studies was employed as the initial source for content adaptation. The researchers used general search engines and scientific databases to identify evidence, continuing their search throughout the study's implementation and reporting phases. One of the strengths of this study is the multidisciplinary nature of the expert panel members and the inclusion of a dedicated panel for people with lived experience. Additionally, the study's focus on a topic with limited similarity to internal studies on EDs adds to its uniqueness and value.
Practical recommendations
Further studies are needed to evaluate the effectiveness of this guideline, the duration of its effects, and its shortcomings. Additionally, updating the guidelines should be a priority for the country's health system. Future revisions should incorporate feedback from various scientific associations dealing with EDs to enhance the comprehensiveness of the guidelines and address all cases, including those with specific complications. Future studies are recommended to conduct pilot, qualitative, and further Delphi studies to measure the effectiveness of the localized guideline, gather feedback, and revise the content based on up-to-date evidence.


留言 (0)