
記住我




The retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [10]. The ethics was approved by the Ethics Examining Committee of Human Research of Beijing Xuanwu Hospital, Capital Medical University (xw-ky-2023109). Written informed consent was obtained from all participants.
Patients admitted to the Pain Department of Capital Medical University Beijing Xuanwu Hospital and underwent TFSIs for the treatment of lumbar radicular pain between January 1, 2022, and September 30, 2023, were screened through the electronic medical records (EMRs). Inclusion criteria were as follows: (1) diagnosis of chronic LBP according to guideline from the American College of Physicians and the American Pain Society [11] and presenting unilateral radicular pain secondary to a lumbar herniated disk (LHD) or foraminal stenosis resulting in symptoms of L5 radiculopathy, (2) confirmation of a LHD or foraminal stenosis at the ipsilateral L5 level by CT or magnetic resonance imaging (MRI), (3) clinical symptoms did not respond to commonly used conservative treatments for at least 6 weeks [12], and (4) ipsilateral iliac crest exceeding the midpoint of the L5 pedicle based on the lateral radiography [0]. Patients were excluded if they had BMI ≥ 30 kg/m2, a history of surgery on the lumbar spine, chronic psychiatric illnesses, convention to other invasive treatments, and incomplete medical data or lost to follow-up.
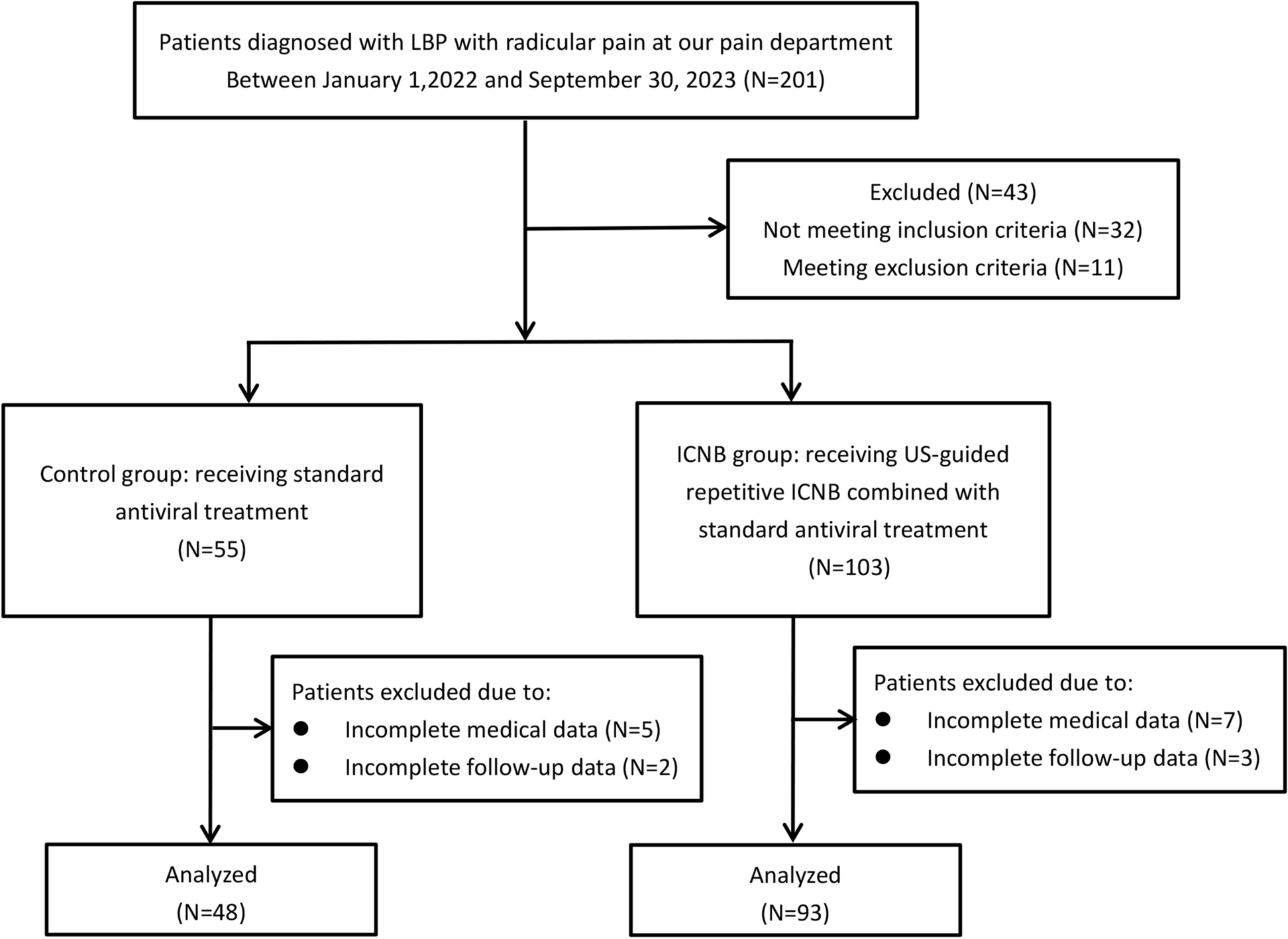
A total of 141 consecutive patients were divided into two groups based on the approach used during US guidance: the novel group, receiving US-guided PRF on the L5 nerve root using the novel approach and verified by FL, or the control group, receiving the same treatment using the transverse method during US guidance (Fig. 1).
Fig. 1
The flow chart of the study
Procedure managementThe procedures were performed by the same team of pain physicians, who were with more than 5 years’ expertise in interventional techniques for chronic spinal pain. All patients were prepared in a prone position with a pillow under the lower abdomen to compensate for the lumbar lordosis in the sterile operating room and monitored by electrocardiography (ECG), noninvasive blood pressure, and pulse oximetry (SpO2).
Novel groupAfter sterilization, a 2–5-MHz curvilinear probe (Labat, Shenzhen Huasheng Medical Technology Co., Ltd., China) was longitudinally positioned on the midline to visualize the targeted segment of L5 spine. A funnel-shaped hyperechoic structure posterior to the dorsal dura was consequently identified between the L5 spinous process (SP) and the S1 sacral crest. By moving the probe further towards the lateral, the hyperechoic funnel situated between the L5 lamina and the sacrum gradually became smaller in sequence (Fig. 2a). Until it completely disappeared, the facet joint of L5–S1 appeared as a hyperechoic line known as the “camel’s hump” with its acoustic shadowing beneath on the sonographic long-axis view (Fig. 2b). Subsequently, the probe was moved to the opposite direction targeting at the inside border of superior articular process (SAP) of S1 (Fig. 2c). After completion of the longitudinal scanning, the probe was then turned about 45° to the ipsilateral iliac crest to gain an oblique line, taking a successional visualization of the unique funnel-like hyperechoic signal lying at the lower inside margin of the S1-SAP as a reference point. In this oblique view, typically, the posterior side of the targeted L5 foramen was identified under the uninterrupted hyperechoic bony line of the S1-SAP (Fig. 2d). Color Doppler mode was manipulated to avoid the critical vessels including radicular or segmental vessels adjacent the puncture path [13]. The needle (Nerve Block Needle, 22G, 15 cm, Shenzhen Huasheng Medical Technology Co., Ltd., China) was advanced towards the outer edge of the targeted hyperechoic line and gently slipped beside it until the loss of resistance (LOR) was achieved using an in-plane approach. The precise position of needle tip was adjusted by advanced a little deeper and not beyond the 6 o’clock position of the vertebral pedicle under FL without contrast medium confirmation. Upon negative aspiration, contrast spread pattern was then verified followed by further injection of 1 ml of contrast medium. A test injection was administered with 0.5 ml of 1% lidocaine. A total of 2 ml of mixture including 0.5 ml of 2% lidocaine (20 mg/ml) and 1 ml of betamethasone (5 mg:2 mg/ml) was subsequently injected.
Fig. 2
a Ultrasound pictures showing that a funnel-shaped hyperechoic structure (solid arrow) was consequently identified between the spinous process (SP) of L4 and L5 and the sacrum on the paramedian longitudinal scans. b The facet joint of L5–S1 appeared as a hyperechoic line known as the “camel’s hump” until the funnel-shaped hyperechoic structure completely disappeared. c The lateral position of the transducer at the inside border of S1-SAP (superior articular process). d By rotating the transducer about 45–60° from the final longitudinal scanning towards the ipsilateral iliac crest with a successional visualization of the unique funnel-like hyperechoic signal lying at the lower inside of S1-SAP, the needle (open arrow) was advanced to the targeted L5 foramen under the uninterrupted hyperechoic bony line of the S1-SAP using an in-plane technique. e and f Fluoroscopic anteroposterior and lateral view verified an intraforaminal contrast dispersion in patients with high iliac crest following the ultrasound-guided novel approach
Control groupAfter identifying the L5 spinal level in the same sagittal US image as the novel group, the curvilinear probe was placed perpendicular to the long axis to view the SP, lamina, facet joints, and transverse process (TP) in sequence. The probe was slightly moved upward or downward to detect the root portions of TP, in which image the posterior edge of the L5 neural foramen was delineated as a hyperechoic bone structure with its underlying acoustic shadow. After confirmation of no critical vessels adjacent the peri-radicular area by color Doppler mode, the same needle as the novel group was positioned from the lateral to the middle using the transverse axis in-plane approach under the real-time US guidance. The precise position of needle tip was then adjusted and confirmed under FL. If the L5 neural foramen was difficult to reach due to the HIC, the procedure might be terminated by administering an agent around the nerve root. The contrast-spread distribution was also verified following the negative aspiration. After the same test injection was confirmed fluoroscopically, the same mixture as the novel group was injected.
Outcomes measurementAll data were collected through the EMRs. Pain severity was assessed by the numerical rating scale (NRS) ranging from 0 (no pain) to 10 (worst pain). Successful treatment response was defined as pain relieving ≥ 50% reduction from baseline NRS score at 1 week after the initial injection on the basis of clinical consensus. Patients reported < 50% reduction in pain relief received the second injection following the same protocol as the first one. Modified Oswestry Disability Questionnaire (MODQ) scores were employed to measure the LBP-related functional disability, where higher scores indicated greater limitation. It consists of 10 items addressing personal care, lifting, walking, sitting, standing, sleeping, social life, traveling, and employment/homemaking. Each item is scored from 0 (no disability) to 5 (maximal disability) [14]. Contrast media dispersion patterns were judged by FL, which were graded as follows: (1) “intra-muscular” type when contrast accumulated locally in muscles without peri-radicular filling, (2) “peri-radicular” type when contrast spread only along the nerve root but not reaching the articular pillars, and (3) “epidural” type if contrast spread exceeding the outer margin of the articular pillars. Procedure time was defined as starting from the ultrasound probe touching the skin of the effective area to the end of the injection. Number of needle insertions and attempts until contrast was given, and radiation dosages, complications, and rescue analgesia were also recorded.
The primary outcome was the accuracy of needle tip placement, as confirmed by the contrast-spread pattern of “epidural type.”
Sample size calculationSample size was calculated using PASS software version 16 (NCDS, LLC, Kaysville, UT, USA) before patients’ screen for eligibility. Because of no certain evidence about the accuracy of TFSI at L5 level using transverse approach under US guidance in patients with high iliac crest, the sample size calculation was based on consensus after a series of expert discussion meetings estimating a 75% accuracy rate. We would like to decide that the novel approach would be adopt if it has an accuracy rate of at least 85%. Using the one-sided Farrington and Manning likelihood score test to reach a power of 90% at group sample size ratio of 2, we came up with 44 patients in control group and 88 cases in novel group, when the difference of the actual accuracy rate between two approaches ranged from 20 to 25%.
Statistical analysisStatistics were performed using a SPSS 22.0 (SPSS Inc, Chicago, IL, USA). Significance was accepted at p < 0.05. Kolmogorov-Smirnov Z-test was performed for the normal distribution of all data. Categorical data, normal distribution data, and non-normally distributed data were expressed as frequencies/percentages, mean ± standard deviation (SD), and median ± interquartile range (IQR) and compared using the chi-squared test, Student’s t-test, and Mann-Whitney U-test between groups. Changes in NRS scores and MODQ scores were assessed using the generalized liner mixed model (GLMMs) taking age, gender, BMI, and iliac height as covariance. Paired and independent t-test derived from GLMMs for repeated measurements were applied for within-group and between-group comparisons, respectively.
留言 (0)