Root canal treatment is a reliable and effective dental procedure for apical periodontitis, a common inflammatory disease of the tooth pulp and surrounding tissues.28 Despite new technologies and techniques, such as advancements in endodontic files and intracanal medications, which have improved success rates, the fundamental concept of root canal treatment for apical periodontitis has remained essentially unchanged over the past few decades.29,30 This procedure aims to eliminate the source of infection by removing the diseased tissue and filling the root canal with an inert material to prevent further bacterial growth.31 Therefore, there are pathways to new materials to be developed, especially those like endogenous human compounds, as they can facilitate healing and tissue regeneration while reducing the risk of infection.
Developing drugs that resemble endogenous molecules is crucial due to their higher biocompatibility with the human body since these compounds are more likely to be recognized and utilized by the body in a beneficial way that minimizes adverse effects. Moreover, these drugs can facilitate the study of biological pathways and mechanisms, ultimately leading to a better understanding of the underlying biology of a disease and more targeted therapies. Thus, developing endogenous-like drugs is a promising strategy that can lead to safer, more effective, and more targeted therapies.13 In this study, we developed and investigated the effect of an HDL-mimicking compound that imitates the structure and function of endogenous natural HDL, using it for apical periodontitis treatment. The murine RAW 264.7 cell line was chosen for in vitro assays evaluating endodontic inflammation over primary cell lines due to its consistent and reproducible nature, stable genetic background, and ease of culture. These factors ensure standardized experimental conditions and reliable results while enabling researchers to perform more experiments with less effort. These cells respond to pro-inflammatory stimuli analogous to primary macrophages, making them a suitable model for studying the inflammatory response in endodontic scenarios.32,33
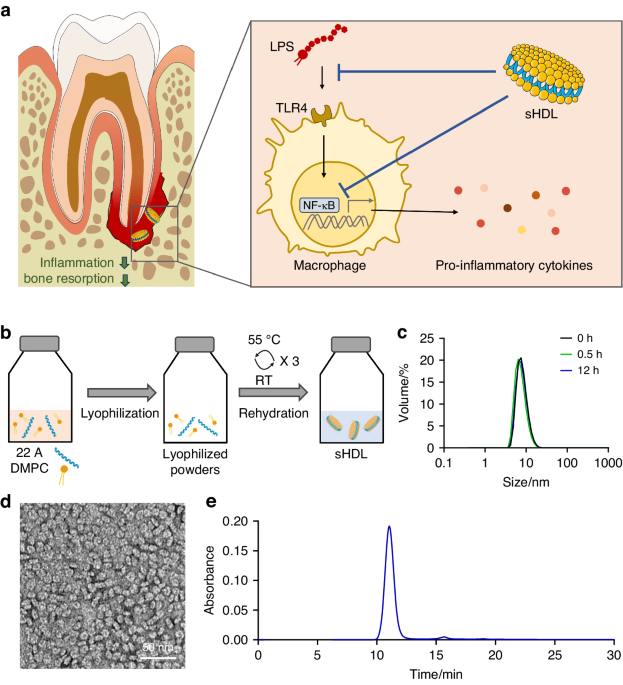
Essential to the pathogenesis of apical periodontitis, lipopolysaccharide is characterized as a pathogen-associated molecular pattern (PAMP) and a potent endotoxin found in the outer membrane of gram-negative bacteria that can cause a range of inflammatory responses by activating the TLR pathway, specifically TLR4, leading to the release of pro-inflammatory cytokines and chemokines.34 Therefore, evaluating the TLR pathway in an LPS-induced infection or inflammatory disease is critical since it can provide insights into the molecular mechanisms underlying the host’s response to bacterial infections and help identify the key signaling components involved in LPS recognition and the downstream inflammatory response, and can aid in developing targeted therapies aimed at modulating TLR signaling and mitigating the inflammatory response.
Activation of the NF-κB transcription factor is a subsequent event due to LPS binding to TLR4 and has been shown to modulate the expression of various pro-inflammatory cytokines, including upregulation of IL-1α, which is a potent pro-inflammatory cytokine that is involved in the pathogenesis of many inflammatory diseases.35 In addition, it induces the expression of IL-6, a pleiotropic cytokine involved in various physiological and pathological processes, including immune response, inflammation, and oncogenesis.36 IL-6 also activates NF-κB signaling, creating a positive feedback loop that amplifies the inflammatory response.37 Overall, the modulation of IL-1α, TNF-α, and IL-6 expression by NF-κB activation highlights the complex interplay between NF-κB signaling and the immune and inflammatory responses.38 In the literature, it is well established that sHDL inhibits the NF-κB pathway through multiple mechanisms. These mechanisms include interference with TLR signaling, lipid rafts modulation, cholesterol efflux promotion, anti-inflammatory and antioxidant properties, and direct interaction with NF-κB signaling components. These actions collectively contribute to the anti-inflammatory effects of sHDL and its potential therapeutic benefits in various inflammatory diseases.18,39,40 Through our luciferase assay, we appreciate the ability of sHDL to inhibit the NF-κB activation by LPS, as well as the diminished production of IL-6 by ELISA, which could also support and explain the less inflammatory profile found in vivo.
Furthermore, LPS can also directly influence the activity of osteoclasts, cells responsible for bone resorption. LPS can increase the expression of receptor activator of NF-κB ligand (RANKL) on osteoblasts, which promotes osteoclast differentiation and bone resorption.41 This can contribute to the bone loss often observed in apical periodontitis. An interesting finding in the present investigation was that the sHDL administration decreased osteoclast formation in vitro dose-dependently from 50 to 500 µg/mL, later confirmed by decreased lesion size through microtomography from our in vivo model. However, when we raised the concentration to 1 000 µg/mL, this reduction pattern reverted to a slight increase, although statistically significantly smaller than the group without sHDL. Such a phenomenon may be attributed to the cytotoxicity of sHDL at high concentrations. Our previous studies suggested that sHDLs had no negative effects on the viability of RAW264.7 cells with concentrations below 100 μg/mL.42 However, high sHDL concentrations, such as 1000 μg/mL, may lead to cytotoxicity due to excessive cholesterol efflux. Moreover, according to the literature, high cholesterol or HDL levels can activate inflammatory factors that increase bone turnover, leading to a decrease in bone mass, suggesting that the use of sHDL must depend on well-defined and precise concentrations so that it inactivates the LPS, hindering the RANKL binding to RANK and subsequent osteoclastogenesis.43,44
Our extensive gene expression evaluation through the TLR PCR array showed that several were upregulated when the sHDL was applied with the LPS. The most upregulated Muc13 gene encodes a transmembrane mucin called Mucin 13, expressed in immune cells such as macrophages and dendritic cells. Although the precise function of Mucin 13 is not fully understood, evidence suggests that it regulates inflammation and promotes tissue repair by preserving the epithelial barrier’s integrity and preventing the entry of inflammatory agents such as LPS. This mechanism leads to decreased production of pro-inflammatory cytokines and chemokines, ultimately reducing inflammation.45
Another overexpressed gene was the interferon regulatory factor 3 (Irf3), a constitutively expressed transcription factor critical in the innate immune response to infections. Irf3 activation leads to the production of type I interferons and promotes the activation of immune cells, including macrophages.46,47 Besides that, Irf3 has been found to have anti-inflammatory abilities since Irf3-deficient mice showed exacerbated inflammation in various models of inflammatory diseases, indicating that its activation could limit inflammation.48,49 Additionally, Irf3 has been implicated in regulating macrophage polarization, with Irf3 activation favoring a shift toward an anti-inflammatory M2 phenotype. In contrast, loss of Irf3 led to an increase in pro-inflammatory M1 macrophages. Therefore, Irf3 not only plays a crucial role in immunity but also possesses anti-inflammatory abilities and macrophage polarization capabilities, making it a potential therapeutic target for inflammatory diseases.49,50
Also upregulated, the Il12a gene encodes a subunit of the cytokine Interleukin 12. While this gene is primarily known for up-regulating inflammatory responses, evidence suggests it also has anti-inflammatory properties, mainly inhibiting the proliferation of pro-inflammatory effector T helper cells. Furthermore, in vitro studies have shown that IL-12 can suppress the differentiation and function of mature osteoclasts induced by the RANKL. When looking at the overall pathogenesis of apical periodontitis in vivo, the endogenous effects of IL-12 do not appear significant.51,52,53,54
Contradictorily, the administration of sHDL increased the expression of Irak1, which stands for Interleukin-1 receptor-associated kinase 1, a serine/threonine protein kinase that plays a critical role in the immune response. This kinase is involved in the signaling pathways activated by TLRs and interleukin-1 receptors (IL-1Rs) that are present in immune cells and recognize PAMPs or damage-associated molecular patterns (DAMPs), triggering a cascade of signaling events that lead to the activation of transcription factors, such as the NF-κB pathway and the MAPK pathway, which culminate and the production of pro-inflammatory cytokines.55
Amongst the fourteen genes downregulated, the three most numerically and statistically significant genes were Il1b, Il1a, and Ccl2. IL-1β and IL-1α are strong pro-inflammatory cytokines regulating immune response and inflammation. Both IL-1β and IL-1α are produced by various cells, including immune cells such as macrophages and dendritic cells, in response to inflammatory stimuli such as bacterial or viral infections.56 The novelty of our approach was to use sHDL as a treatment for apical periodontitis. While our animal model exhibited no significant differences in the immunolabeling of IL-1β and IL-1α compared to the currently standardized treatment (NaOCl + Ca(OH)2), it effectively reduced the expression of both pro-inflammatory interleukins compared to untreated groups. Our PCR array analysis yielded similar results, with these two interleukins being the most downregulated, suggesting that the observed anti-inflammatory effect in histology is primarily attributable to the modulation of these two proteins compared to SHAM.
The Ccl2 gene, which encodes the C-C motif chemokine ligand 2 protein (also known as monocyte chemoattractant protein-1 or MCP-1), is produced by a variety of cells including macrophages, endothelial cells, and smooth muscle cells, in response to pro-inflammatory stimuli such as cytokines and LPS. It has been found to promote chemotaxis, differentiation, activation of osteoclasts, and perpetuation of the inflammatory response. Moreover, a study has demonstrated that in the presence of RANKL, MCP-1 significantly increased the number of TRAP-positive multinuclear bone-resorbing osteoclasts in vitro,57 and a previous investigation using an in vivo model demonstrated the increased expression of MCP-1 in the apical lesion that can elicit pro-inflammatory cytokines, such as TNF-α and IL-1β, which can further perpetuate the inflammatory response and contribute to tissue destruction.58 This highlights the potential of sHDL since it targets the Ccl2, and its downstream effects may be a potential therapeutic approach for treating apical periodontitis.
Another explanation for how the sHDL promotes the anti-inflammatory effects can be linked to the upregulated gene expression of Ppara (Peroxisome Proliferator-Activated Receptor alpha) and Fadd (Fas-Associated protein with Death Domain) found in our PCR array. Ppara and Fadd play crucial roles in regulating inflammation, although through different mechanisms. Ppara is a nuclear receptor that modulates gene expression involved in lipid metabolism and inflammation by binding to c-Jun and to the p65 subunit of NF-kB. Activation of Ppara by fatty acids or synthetic agonists suppresses inflammatory responses by inhibiting the expression of pro-inflammatory genes and promoting the expression of anti-inflammatory genes.59,60Fadd, known for its role in apoptosis signaling, may negatively regulate the TLR4-NFκB axis by interfering with MyD88 (myeloid differentiation primary response 88), a crucial adapter protein in TLR4 signaling. Upon TLR4 activation by ligands like LPS, MyD88 is recruited, initiating a cascade leading to NFκB activation and further pro-inflammatory cytokines like IL-1α and IL-1β production. FADD’s interaction with MyD88, likely facilitated by their death domains, could disrupt the formation of active signaling complexes necessary for NFκB activation, thus dampening the immune response. Additionally, FADD’s pro-apoptotic function might contribute to this negative regulation by promoting cell death, providing a potential feedback mechanism to prevent excessive or prolonged immune activation and inflammation-associated pathology.61 Overall, our findings demonstrated that sHDL could effectively control the inflammatory reaction and bone resorption associated with apical periodontitis by upregulating Ppara and Fadd and reducing the expression of proinflammatory cytokines, suggesting a partial inhibition of the TLR pathway.
Translating to the clinical approach, manually preparing calcium hydroxide before its application inside the root canal is a cost-effective option. However, in pursuit of enhanced ease of use, pre-mixed calcium hydroxide in syringes has entered the market as a more convenient but slightly pricier alternative. Also, calcium hydroxide injection directly into the periradicular area, a common occurrence in cases of immature apexes, perforations, or close proximity to neurovascular structures such as the inferior alveolar nerve and its mental distribution (typically associated with mandibular posterior teeth), poses severe risks to patients. The highly alkaline nature of calcium hydroxide can lead to inflammation and irreversible damage to surrounding tissues, including bone and soft tissues, resulting in complications such as paresthesia, dysesthesia, and necrosis. Furthermore, extruded calcium hydroxide lacks systemic absorption capability and may cause significant harm if it enters the bloodstream.62
In this way, our sHDL technology represents a novel and safer approach since it resembles an endogenously produced molecule of the body. Understandably, it comes with a higher price tag than existing materials. Nevertheless, as the application of this advanced technology becomes more widespread, manufacturing costs are expected to decrease, not adversely affecting the overall price of root canal treatments, ensuring accessibility and affordability for patients. Our findings shed a green light on the potential use of pure HDL-like carrier as a therapeutic agent for apical periodontitis and pave the way to improve it by loading the nanoparticle core with drugs or other therapeutic agents that target specific tissues or cells, potentially enhancing the efficacy of certain medications while minimizing side effects. Since this is the first study evaluating this lipoprotein for endodontic treatment, we can point out some limitations, such as using a small animal model and the absence of sHDL residence and stability time assessment when locally administered to teeth. Thus, further studies that evaluate these parameters coupled to a larger animal model, such as canine or porcine, are crucial to bringing us closer to replicating a clinical scenario in human teeth and refining carrier systems to enhance the delivery of sHDL.




留言 (0)