
記住我


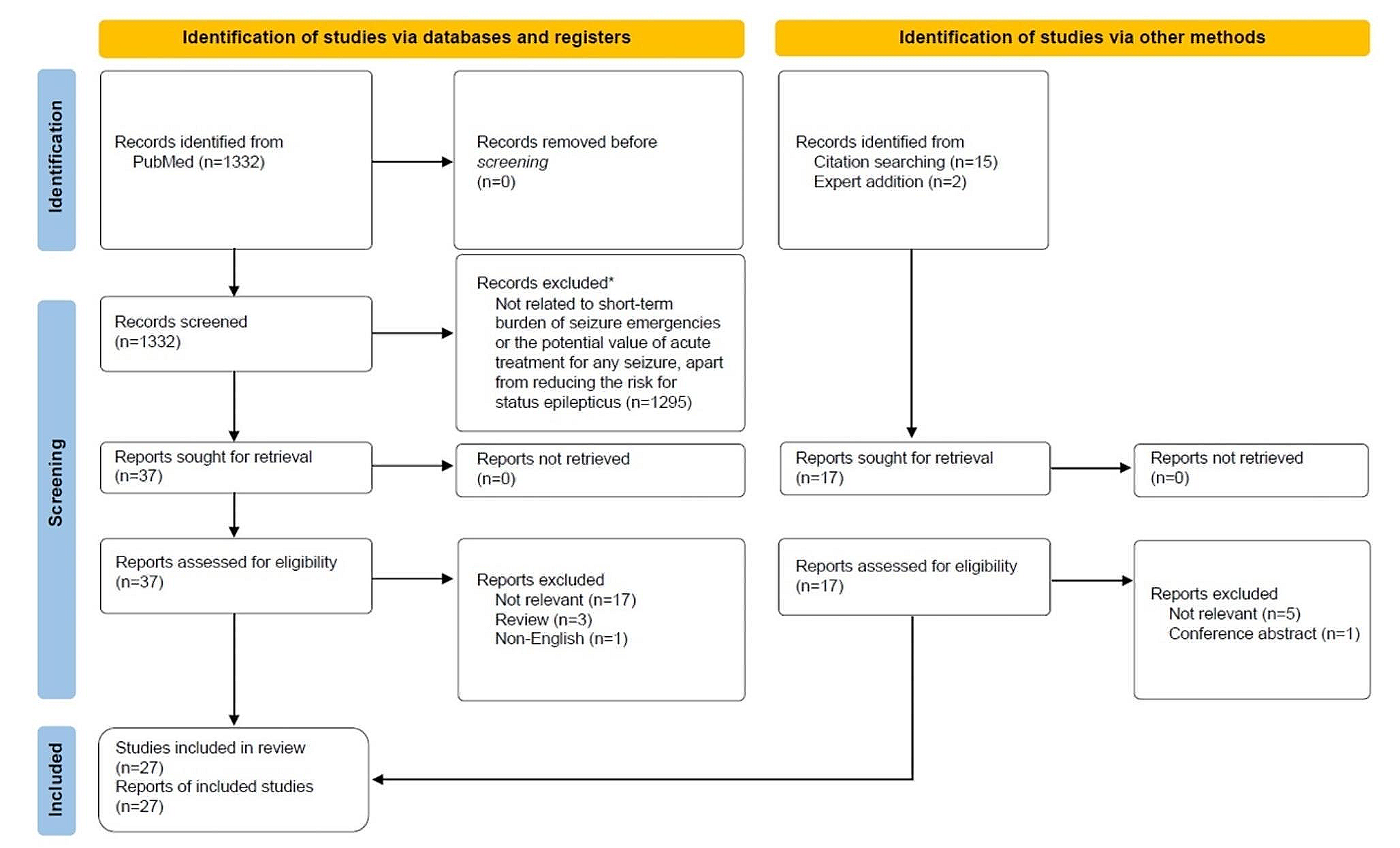
A total of 1332 articles that met search criteria were screened, and 37 articles were selected for full-text review. An additional 17 articles were identified through other methods, including citation searching and expert addition. After eliminating duplicates, a total of 27 articles were included in the qualitative synthesis (Fig. 1; Table 1); 13 articles presented outcomes related to short-term seizure burden [2,3,4,5, 11,12,13,14,15,16,17,18,19], 13 articles presented outcomes related to acute seizure treatments to reduce short-term seizure burden [20,21,22,23,24,25,26,27,28,29,30,31,32], and 1 article presented outcomes on both [33].
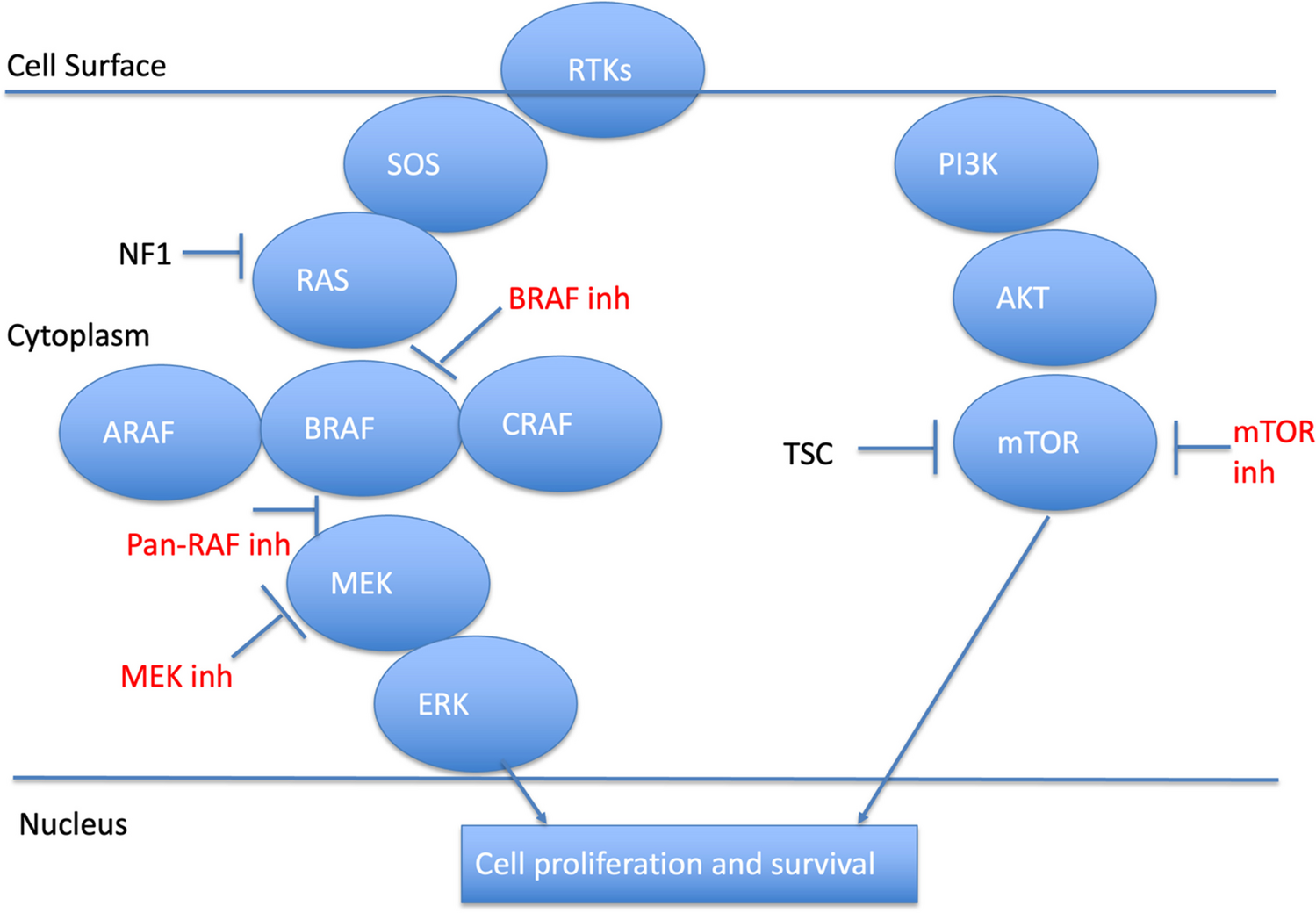
Fig. 1
PRISMA chart. *The following article types were excluded: review (systematic, narrative), letter to the editor, correspondence, editorial, and opinion articles that did not present original data. Additionally, articles related to the general burden of epilepsy (e.g., depression) were excluded, as were articles that pertained to certain consequences of acute seizures (e.g., drowning) for which the impact might not be expected to be modified through the use of acute treatments
Table 1 Study characteristicsBurden of Acute SeizuresQuality of Life/Daily ActivitiesSeizure severity, of which seizure duration is a key component, constitutes a substantial aspect of seizure burden [4]. In addition to negative outcomes directly related to the seizure (e.g., injuries, emergency services), the acute burden of seizures includes the interruption of activities or normal routines as well as managing the emotional and social aftermath of a seizure (e.g., cleaning up, trauma to others, embarrassment) [4]. In a survey of patients with seizure clusters, 71% reported lowered expectations to conduct daily activities, and 68% believed that these seizure emergencies got in the way of performing their daily responsibilities [5]. 70% of patients felt that seizure clusters had a moderate to major negative impact on quality of life, 54% reported that they worry about a loss of seizure control in public, and 75% somewhat or strongly agreed that they live in fear that a seizure will occur at any time. 68% of patients worry about a loss of independence, and more than half of the patients indicated that seizure clusters make them feel exhausted (76%), stressed (63%), or depressed (62%). Additionally, seizure clusters affected employment and school attendance/performance for 69% and 32% of patients, respectively. A majority of patients indicated negative impacts of seizure clusters on the ability to participate in extracurricular (58%) or social activities (57%), and 59% felt that clusters negatively affected their ability to travel [5].
In a cross-sectional study, health-related quality of life assessed with the EuroQoL-5D instrument was very low in children and adolescents who experienced prolonged acute convulsive seizures (PACS) compared with adults (mean scores of children/adolescents with PACS rated by clinicians [0.52], parents [0.51], and patients [0.74] vs. adult population norm [0.86]) [13]. Seizure-related injuries also can negatively affect quality of life [18, 19]. In a retrospective study conducted at an epilepsy outpatient clinic, injured patients had decreased overall quality-of-life scores compared with uninjured patients (mean QOLIE-31 T-score; 38.9 vs. 49.2, respectively; P < 0.001), including greater seizure worry (P ≤ 0.001) and reduced social function (P < 0.001) [18]. In a separate retrospective study, injured patients had reduced quality of life compared with uninjured patients (mean QOLIE-31 score; 36.5 vs. 55.6, respectively; P = 0.002), as well as greater levels of seizure worry (Cambridge Worry Scale; 5.3 vs. 4.3, P = 0.008) [19].
Physical BurdenAcute seizures can lead to accidents and injuries, such as fractures, head trauma, joint dislocations/sprains, and burns [2, 11, 14, 18]. In a retrospective, single-center study that examined seizure-related injuries, the most common injury type was fracture (49%), followed by head trauma (27%) and soft tissue injuries (24%) such as lacerations, joint dislocations, and sprains; 29% of patients required intensive care [2]. In a retrospective study that evaluated patients at epilepsy centers in controlled conditions who were monitored with video and electroencephalography, serious adverse events (e.g., fractures, joint dislocation, eye abrasions, tooth loosening) associated with generalized convulsive seizures occurred in 13 patients (3%); 1 had a fall-related serious adverse event [17]. Additionally, 12% of patients experienced minor physical injuries (e.g., tongue/lip biting, lacerations) [17]. A prospective study found that 16% of patients from a comprehensive epilepsy center outpatient clinic experienced a seizure-related injury over a 1-year follow-up [33]. In another study conducted at an epilepsy outpatient clinic, 14% of patients had injuries attributed to epilepsy during a 3-month period, and 7% of patients were hospitalized as a result of injury [18]. In a retrospective study of women with epilepsy, 13% experienced injuries related to epilepsy during the 3-month study period [19]. The most commonly reported injuries were laceration; abrasion, cut, bruise or hematoma; burns; fracture; and severe tongue bites. Predominant seizure type (focal tonic or clonic, generalized tonic-clonic, or only automotor seizures) was not associated with injury [19]. Shoulder dislocation can occur during a seizure, and chronic dislocation can lead to damage of articular cartilage, bone, and neurovascular structures, resulting in persistent pain, stiffness, and reduced range of motion [11, 14]. In a retrospective study conducted at a university hospital (neurology and surgery/orthopedics departments), 1% of patients over an 8-year period who experienced an acute bilateral tonic-clonic seizure also had an acute shoulder dislocation, and these patients constituted 5% of all patients (any etiology) treated for acute shoulder dislocations [14].
Financial BurdenPatients might seek professional medical care (e.g., emergency medical services, emergency department [ED] visit) for treatment of acute seizures, in part, because of a lack of education (e.g., have not had a discussion about home management as outlined by an individualized seizure action plan) to manage the episode [5]. In a survey of patients with seizure clusters, most patients (24%) indicated that they would visit the ED for treatment compared to taking rescue medication (20%) or calling their doctor (20%) [5]. In some school settings, however, administrative policies may require a call for emergency services even if rescue medication was administered [32]. In a prospective study of patients with epilepsy, 17% reported seizure-related ED visits over a 1-year period [33].
One regional study of emergency calls for convulsions/seizures in the United Kingdom estimated that total costs in England for prehospital ambulance care of acute seizures could be as high as £9.8 million per year in 2012 (~$15.5 million USD) [16]. In a retrospective cohort study that used commercial and federal (United States, Medicare/Medicaid) claims data from 2013/4 to 2017/8, the median cost for an epilepsy-related hospitalization in commercially insured patients was $22,305, and the median length of stay was 4 days (in patients of working age [19–64 y]) [3]. Median costs for epilepsy-related hospitalizations for Medicaid- and Medicare (with supplemental insurance)-insured patients were $9837 and $19,577, respectively [3]. In a separate study using US commercial and Medicaid data from 2010 to 2015, the average cost per seizure event (as determined through International Classification of Diseases codes, 9th Revision [ICD-9] for epilepsy or convulsion; recorded upon admission to the ED or inpatient clinic that originated in the ED) ranged from $8147 to $14,759 in patients with Lennox-Gastaut syndrome, $4637 to $8751 for those with Dravet syndrome, and $5335 to $9672 for those with tuberous sclerosis complex [15].
Additionally, absenteeism from work could contribute to the financial burden of acute seizures [5]. In a survey of patients with seizure clusters, among the 69% who reported that seizure emergencies negatively affected their job/career or ability to work, 62% of patients reported having experienced a seizure at work, 53% reported having to stop working completely at some point due to seizures, and 33% felt that their job performance was more closely monitored [5]. Almost half (48%) reported lost employment due to seizure clusters. In a survey of caregivers, 48% indicated that seizure clusters negatively affected their job or career; among caregivers reporting an effect on work, 49% had to reduce time at work, 43% had to stop working for a period of time, and 35% had to disclose the patient’s condition to their employer [5].
Potential Role for Seizure Action PlansSeizure action plans (SAPs) that detail overall seizure management (daily and rescue medications and use, first aid, special instructions, contact information), as well as acute seizure action plans (ASAPs) that focus specifically on acute management of seizure emergencies, may reduce the short-term burden of seizures [23, 34]. SAPs may increase caregiver knowledge [21, 22] and comfort with seizure care [24] and can educate and empower patients, family members, and caregivers to self-manage seizure emergencies (standard first aid, when and how to administer rescue medication, when emergency services should be called). There are no studies that directly examine whether SAPs specifically reduce healthcare resource utilization; there is some indirect evidence from 2 studies of pediatric patients with epilepsy [24, 25]. In these studies, pediatric patients who received an SAP either had more follow-up clinic visits [25] or were less likely to miss a clinic visit [24] than patients without an SAP. In a separate study of pediatric patients, the completion of an SAP and availability of rescue medication at school in addition to the implementation of 5 other interventions were associated with a reduction in ED visits from 13% to 10% per 1000 patients over a 4-year period from project initiation [30].
An ASAP is designed to provide easy-to-understand instructions to care for seizure emergencies and to reinforce the proper use of therapy. This allows family members and other caregivers to manage a seizure in the community setting. This potentially reduces the need for emergency transport and hospitalization and possibly then reduces healthcare costs associated with single seizures [23]. The ASAP (Fig. 2) format combines succinct instructions along with graphics to aid in its use during seizure emergencies [23]. Although there are no studies that examine the effectiveness of an ASAP to reduce the short-term burden of seizures, the potential value of an ASAP is supported by evidence associated with the use of action plans in other therapeutic areas (e.g., asthma, COPD), which incorporate similar structural elements (concise wording, color coding, graphics, flow charts) and have demonstrated success to reduce healthcare utilization [26, 27]. Additionally, structured educational programs may be effective to improve acute seizure treatment in home and community settings. One study described the effects of an educational program to improve participant (teachers, social workers) knowledge and attitudes related to acute seizure treatment [20]. After the program, which included training meetings and educational materials (slides, simulations, videos), participant knowledge of how to best manage epileptic seizures improved from 8% before training to 67% after training. Importantly, confidence to administer rescue medication improved from 52% before training to 81% after training [20].
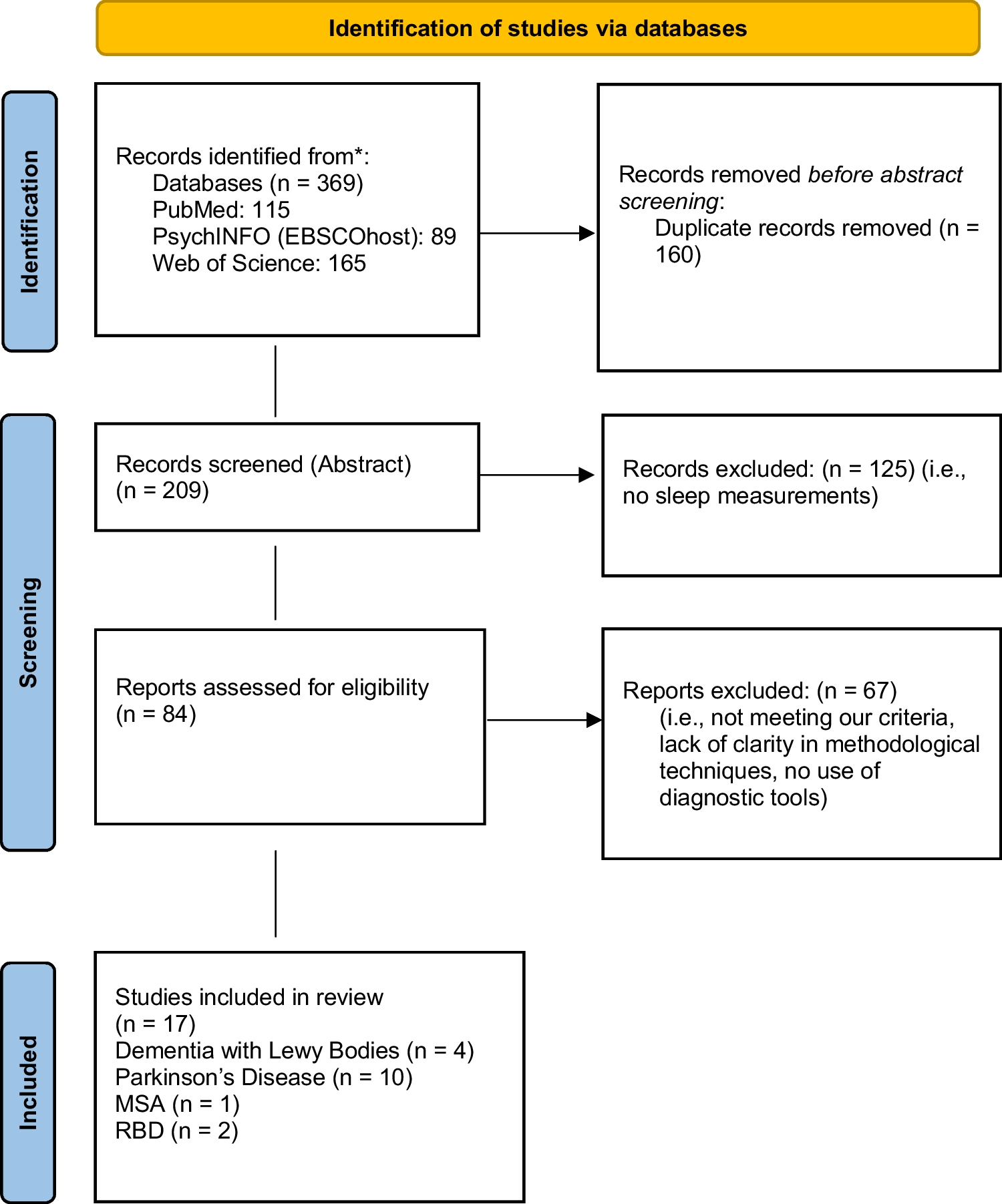
Fig. 2
Acute seizure action plan (ASAP)
Acute Treatment to Reduce Short-Term Burden of SeizuresAcute treatment for seizure emergencies typically includes a benzodiazepine [8] formulated according to the route of administration. Injectable diazepam, lorazepam (both intramuscular and intravenous), and midazolam (intramuscular) are approved by the US Food and Drug Administration (FDA) for status epilepticus [35]. FDA-approved treatments for seizure clusters are diazepam rectal gel (approved in patients with epilepsy ≥ 2 years of age), diazepam nasal spray (≥ 6 years), diazepam buccal film (2–5 years), and midazolam nasal spray (≥ 12 years) [36,37,38,39]. Seizure patterns associated with clusters are distinguishable from a patient’s usual pattern and typically can be recognized by a caregiver [40]. In the European Union, an oromucosal midazolam solution (buccal) is approved by the European Medicines Agency for acute treatment of PACS [35]. Other benzodiazepine formulations (e.g., oral) may be used off-label to treat seizure emergencies [41].
In a survey of patients and caregivers from a long-term safety study of diazepam nasal spray, 38% of patients returned to their usual self within 30 min of receiving diazepam nasal spray, and by 1 h, 59% had done so [
留言 (0)