Currently, ureteral strictures are managed in a variety of ways [5]. Endovascular surgery is often the first choice for clinical physicians because of its minimally invasive nature and rapid associated postoperative recovery [6]. Many studies have shown that in patients with a history of pelvic surgery, endoluminal procedures (be they endotomy, balloon dilation, multiple stent retention, etc.) have poor long-term outcomes and may make patients undergo multiple operations [7,8,9]. Repeated ureteroscopic surgery will not only increase the difficulty of subsequent surgical procedures but also greatly increase the psychological and physiological burden of patients and also increase the economic burden on these patients [10]. Laparoscopic ureteral stricture resection and end-to-end anastomosis have been confirmed to be effective treatment options for such ureteral strictures that occur as a result of pelvic surgery [11]. However, after pelvic surgery, the ureteral stricture is often located and dissociated due to severe scar adhesion and normal anatomical stricture; thus, it can be difficult to free the ureter above and below the stricture. If the normal ureter is injured again during the process of dissociation, it may bring devastating consequences to the normal reconstruction of the ureter [12]. Therefore, accurately locating the ureteral stricture segment, safely dissociating the normal ureteral tissues above and below the stricture segment, and accurately cutting off the ureteral scar are critical to ensuring low-tension anastomosis of the ureter. They are also the difficult parts of the procedure [13].
In order to accurately determine the location of the ureteral stenosis, numerous scholars have tried different methods. Kim et al. [14] used indocyanine green near-infrared fluorescence imaging to accurately locate the narrow segment of the ureter; however, the indocyanine green dye may cause side damage to the ureter. Verbeek et al. [15] used low-dose methylene blue near-infrared fluorescence to guide the identification of ureteral stricture during surgery, however, due to the complexity of these methods, they have not been effectively promoted. There are also reports of scholars using flexible ureteroscopy to locate the ureteral stenosis during surgery, then using robot-assisted laparoscopy to treat lower ureteral stenosis, achieving good results [16,17,18].
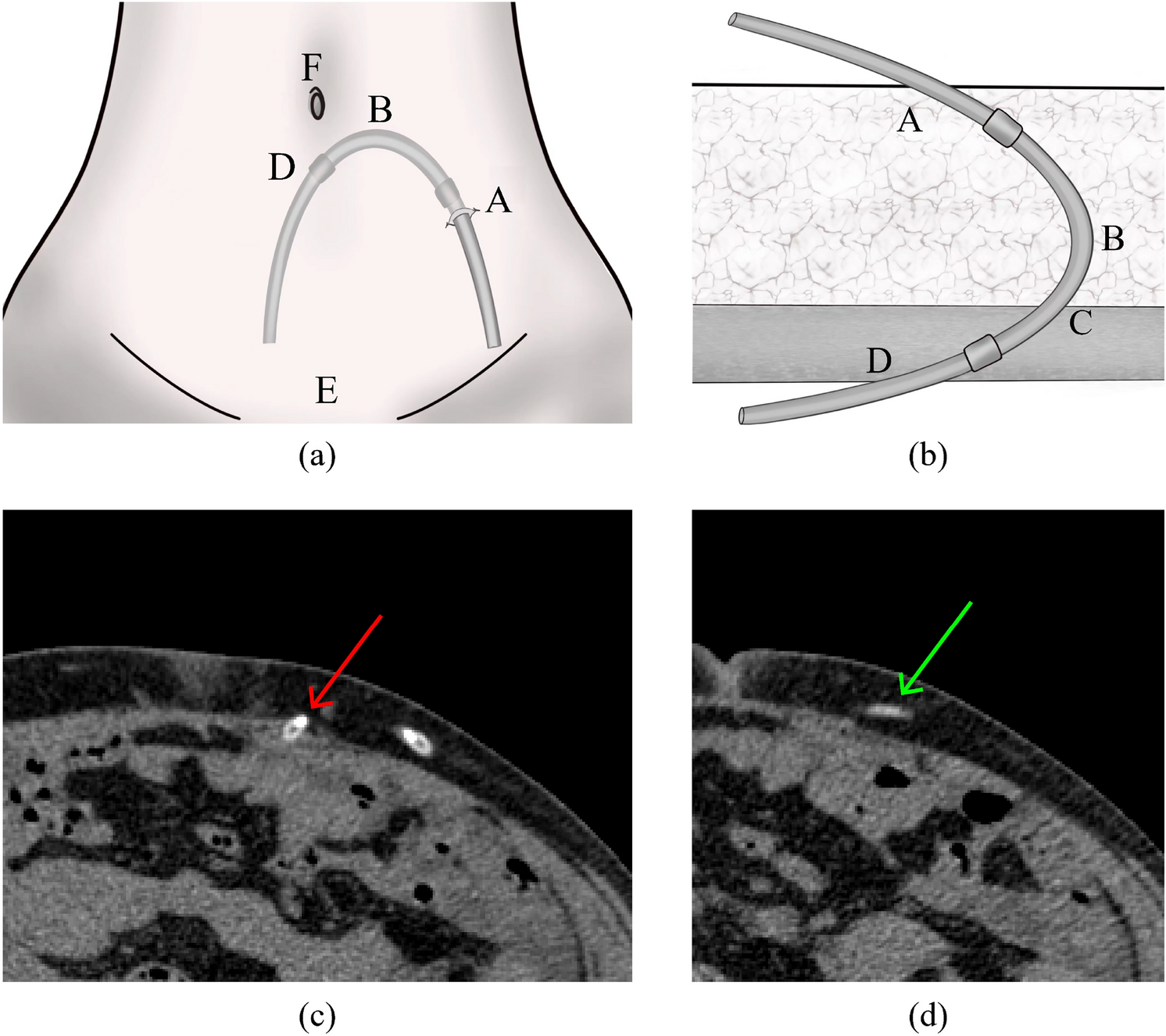
In this study, we carried out laparoscopic ureteroplasty with the aid of a ureteroscope in the lithotomy position (head high and foot low), achieving good therapeutic results. We found during the surgery that freeing the dilated ureter above the stricture was relatively easier, but the ureter at and below the stricture often faced issues due to complications of previous surgeries, including intense inflammation, dense fibrotic scar tissue surrounding the ureter, and loss of normal anatomical structures, making the freeing process difficult [19, 20]. Therefore, after freeing the ureter above the narrow segment, we immediately let the assistant perform a retrograde ureteroscopic procedure from below. When the ureteroscope reached the narrowed segment through the affected ureter, we adjusted the brightness of the room and laparoscopic source to highlight the light from the ureteroscope, then used the guidance of the ureteroscope light and the assistance of the ureteroscope to free the normal ureter at and below the stenosis. The flexible use of ureteroscope can significantly reduce the difficulty of freeing during laparoscopic surgery, preventing further damage to the normal ureter and injury to surrounding organs, ensuring the safety of the surgery. Therefore, in this study, the average operation time and intraoperative bleeding volumes for the observation group were (121.3 ± 44.6) min and (137.5 ± 34.2) ml, respectively, compared to (151.2 ± 52.3) min and (165.6 ± 45.8) ml for the control group. The difference between the two groups is statistically significant.
When trimming the narrow segment, it should not be determined by the brightest location of the light source, but according to the position of the tip of the ureteroscope. Some patients, the narrow segment is not long, and the light can pass through it, where the brightest location is usually the normal ureter location. If the ureter is trimmed according to light intensity, it could inadvertently harm the normal ureter and affect the success rate and effectiveness of the surgery. Our method is to have the assistant press the tip of the ureteroscope against the narrow segment, touch the lens with the laparoscopic scissors, and trim the fibrous scar of the ureter along the front end of the ureteroscope lens, achieving precise trimming. After trimming the distal end of the narrow segment, the proximal end of the ureteral stricture is incrementally trimmed until the urinary flow is seen. During the ureteral suture, the ureteroscope can also play an auxiliary role. The ureteroscope passes through the trimming port and expands the ureteral cavity. When anastomosing the posterior wall of the ureter, the suture needle fastens throughout the ureter wall by following the ureteroscope, which can avoid accidentally encountering the anterior wall of the ureter, achieving precise anastomosis. The support from the ureteroscope is akin to an assistant inside the patient's abdominal cavity: the assistant can moderately swing or push the distal end of the ureter, helping the main surgeon achieve tension-free anastomosis. After the anastomosis of the posterior wall of the ureter is complete, the assistant uses the ureteroscope to retrogradely place a zebra guidewire to the renal pelvis, then withdraws the ureteroscope, and inserts a 7F double J tube retrogradely under the supervision of the laparoscope, ensuring that the ureteral stent is in the most rational position, playing an effective drainage role.
In this study, 49 patients in the observation group successfully underwent laparoscopic ureteral stricture segment resection and end-to-end anastomosis with the assistance of ureteroscopy. Among them, three patients underwent ureteral-bladder implantation due to an inability to perform end-to-end anastomosis because of the normal length of the ureter beneath the free ureteral narrowing segment after gynecological surgery. All surgeries were successfully completed. Only one patient had hematuria postoperatively, which recovered after conservative treatment, the complication rate was only 2%. Clinical symptoms improved, hydronephrosis decreased, and the effectiveness of the surgery reached 100% in the 49 patients followed up postoperatively. In the control group of 46 patients, 2 patients developed urinoma, 1 patient developed vesicovaginal fistula, and 2 patients developed postoperative fever. After the removal of the double J tube, three patients in the control group experienced re-narrowing. The postoperative complication rate was 19.6%, exhibiting a significant statistical difference when compared to the observation group. The surgical success rate and effectiveness rate in the observation group were significantly higher than those in the control group. Thus, it can be seen that ureteroscopy-assisted laparoscopic ureteroplasty can achieve efficient and safe surgical effects.
In this study, we summarized the following advantages of ureteroscopy combined with laparoscopy during ureteroplasty performed in the lithotomy position: first, the lithotomy position is convenient for the combined upper and lower operations required during surgery, and the surgeon and assistant each perform their duties to achieve mutual collaboration. Second, ureteroscopy can help the surgeon accurately dissociate the ureteral stricture segment, accurately locate the position of the ureteral scar, achieve fine tailoring of the stricture scar, and reduce the reduce side injury incurred during the operation. Third, ureteroscopy-assisted laparoscopic surgery can reduce the difficulty and tension of laparoscopic ureteral anastomosis, achieve the normal alignment of the ureteral mucosa and mucosa, avoid the formation of anastomotic scars, and prevent restenosis. Fourth, retrograde indwelling of the double J stent under laparoscopic direct vision and the indwelling zebra guidewire under ureteroscopy are capable of not only ensuring that the ureteral stent is placed in the best position but also saving the time spent on the laparoscopic placement of the double J stent and improving the efficiency of surgery.
However, this research has the following limitations: it is a single-center retrospective study with a relatively low number of surgical patients. Future prospective studies with more extensive data are expected to further confirm the safety and efficacy of this surgical approach.

留言 (0)