
記住我







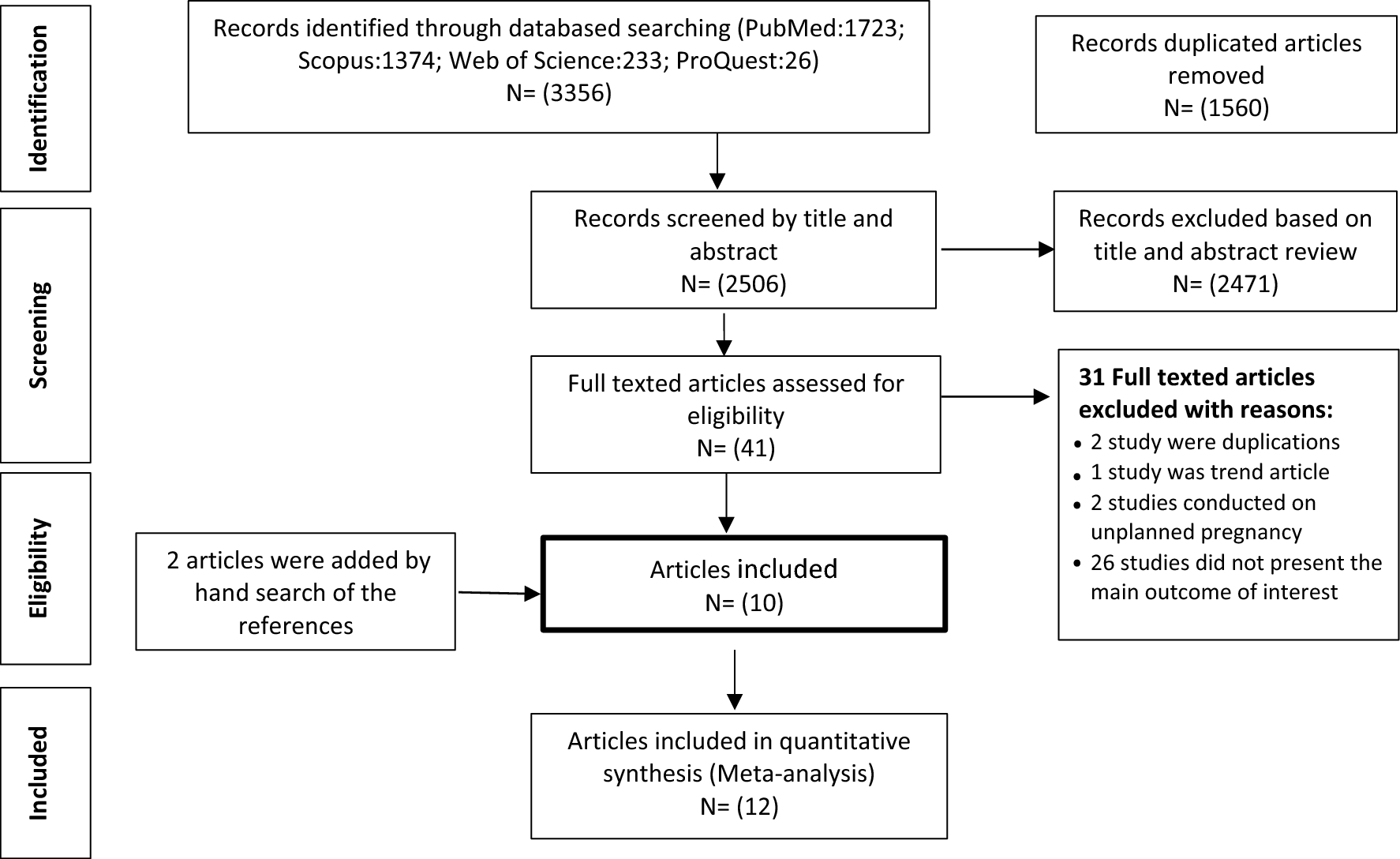

Three hundred seventeen studies were identified through electronic databases (ISI: 104, Scopus: 154, and PubMed: 59). After removing the duplicate studies, the title and abstracts of 177 articles were reviewed, from which 156 articles did not meet the inclusion criteria, and 21 articles were assessed for eligibility. 16 articles were previous versions of included guidelines. Eventually, 5 studies that met the inclusion criteria were retrieved. In addition, 11 guidelines were retrieved through related organizational websites, and after the removal of duplicate guidelines (n = 2), the remaining 14 guidelines that met the inclusion criteria, were included in the review (Fig. 1).
Fig. 1
PRISMA 2020 flowchart of study selection
Guidelines characteristicsFourteen documents were included in this review of which eight were guidelines [30, 43,44,45,46,47,48,49], three were practice codes [34, 50, 51], and three were committee opinions [52,53,54]. Five guidelines were developed in the United States [30, 44, 52,53,54], three Canada [45,46,47], two in the United Kingdom [34, 48], and one in Australia [49] and one guideline in Australia and New Zealand [50] were identified. Also, two guidelines developed by the European Society of Human Reproduction and Embryology (26, 36) were identified. The majority of guidelines (64%) were developed in the last five years (n = 9). Guidelines were also categorized by the research team based on their focus on the gamete and embryo donors. If a guideline specifically was developed regarding gamete/embryo donors, it was considered as totally focused; if the document was about third-party reproduction and included some content related to the recipients and/or donation offspring, it was considered partly focused; and if the guidelines were about infertility treatment in general with some content on donors, it was considered slightly focused. The characteristics of the guidelines are available in Table 1.
Table 1 Characteristics of clinical and ethical guidelines regarding gamete and embryo donorsTwo guidelines were considered of very good quality with overall AGREE II score of 6. Four guidelines were of good quality (overall AGREE II score = 5). While six documents were of poor quality (overall AGREE II score = 3). Also, two guidelines were considered very poor in quality (overall AGREE II score = 2). It must be noted that among the poor-quality documents, there were three committee opinions, which can justify their low score, since some items of the AGREE II tool did not apply to these types of documents. Quality assessment score of each domain and overall score can be found in Additional File 2.
Main findingsFour main categories of management and care provided for gamete and embryo donors were identified including (1) screening (2) counseling (3) information provision and (4) ethical considerations. These categories will be further discussed.
ScreeningAccording to the reviewed guidelines gamete and embryo donors must be screened before donation to ensure the safety and well-being of all parties involved in third-party reproduction. Screening guidelines provide evidence-based eligibility and exclusion criteria for potential donors. Although there are variations among guidelines, the screening process mainly consists of taking medical history, physical exams, infectious diseases screening, genetic screening, and psychosocial screening (Table 2).
Guidelines recommend taking potential donors’ medical history including surgical history and if relevant, the medical history of their family. In such a way, not only ineligible people are excluded but also health-care providers can assess possible risks due to the donation that can influence potential donors’ health based on their medical history [30, 34, 46,47,48].
Physical examination of potential donors including pelvic examination of oocyte donors is also recommended by included guidelines [30, 34, 47, 48].
Based on the reviewed guidelines to minimize the risk of infection transmission among gamete/embryo donors, recipients, and donation offspring; it is important to screen potential donors for infectious diseases [30, 34, 47,48,49,50]. Four guidelines provide detailed recommendations regarding infectious disease, including screening for infectious disease, treatment, re-screening and quarantine period needed for provided gametes and/or embryos before using them in donation [30, 34, 47, 48]. Tests of HIV-1 and HIV-2 antibody, Hepatitis B antigen and antibody (IgG, IgM), Hepatitis C antibody, and serology for syphilis, except of one guideline that recommends it only in sperm donors [46] is recommended for all potential gamete/embryo donors [30, 34, 46,47,48]. While two guidelines recommend routine screening for chlamydia and gonorrhea in all donors [30, 48], CEST’s guideline recommends routine chlamydia and gonorrhea screening only in sperm donors [46], HFEA’s ‘Code of Practice’ advises just routine chlamydia screening only in sperm donors [34], and CFAS’s ‘Guideline on Third-party Reproduction’ recommends routine gonorrhea screening for only female donors [47]. Screening for HTLV types I and II, and cytomegalovirus (CMV) (IgG, IgM) are more controversial. CEST’s guidelines recommend routine HTLV and CMV screening only in sperm donors [46]. CFAS’s ‘Guideline on Third-party Reproduction’ recommends CMV screening in all male donors and HTLV screening in male embryo donors [47]. ASRM’s Guidance regarding gamete and embryo donation recommends CMV and HTLV screening in all male donors [30]. HFEA’s ‘Code of Practice’ advises screening for CMV based on the medical history of the donor and HTLV screening based on both medical history and birth or residing country of donors [34]. Just one guideline recommends routine CMV and HTLV screening in all donors [48].
Some documents recommended additional testing. Both British guidelines recommend further evaluation for infectious diseases such as HPV and HSV based on medical history, if needed [34, 48]. Canadian guidelines recommend ABO and Rh screening in all donors, trachomatis in female donors, and ovarian reserve tests in oocyte donors [47].
Five guidelines recommend completing a comprehensive genetic/heredity disease questionnaire for potential donors and screening them for genetic diseases to exclude potential donors with genetic/chromosomal defects [30, 34, 46,47,48].
It is recommended by some of the included guidelines that fertility clinics establish a mechanism to update and monitor the health status of the gamete/embryo donors including medical and genetic disease history [30, 52].
According to the included guidelines psychosocial and mental health screening of potential donors is another important part of the donation process, and using validated questionnaires and/or tests and interviewing potential donors in order to identify any absolute or relative exclusion criteria is seen as crucial [30, 34, 43,44,45,46,47,48].
Table 2 Screening tests recommended by different guidelines for the potential gamete/embryo donorsCounselingAccording to some of the included guidelines the decision to donate gamete/embryo is complicated and donors would benefit from psychological counseling [30, 34, 51]. In earlier guidelines, counseling was carried out to screen potential donors’ mental/psychological health, but the latest guidelines have separated counseling from psychological screening. These guidelines recommend that counseling should be separated from mental screening and/or information provision [34, 48, 49, 51]. Counseling for donors consists of donation motivation, donation implications on donors’ life, contact with donation offspring, legal issues, time of counseling, providing support, and special concerns (Table 3).
Approaches to counseling vary among countries [51]. As per included guidelines counseling is mandatory for all parties involved in third-party reproduction in Australia, Canada, New Zealand, and the United Kingdom [34, 47, 49, 50]; although counseling is not mandatory in the United States, ASRM strongly recommends it [30].
It has been highlighted in the majority of guidelines that during counseling sessions, the counselor
留言 (0)