
記住我







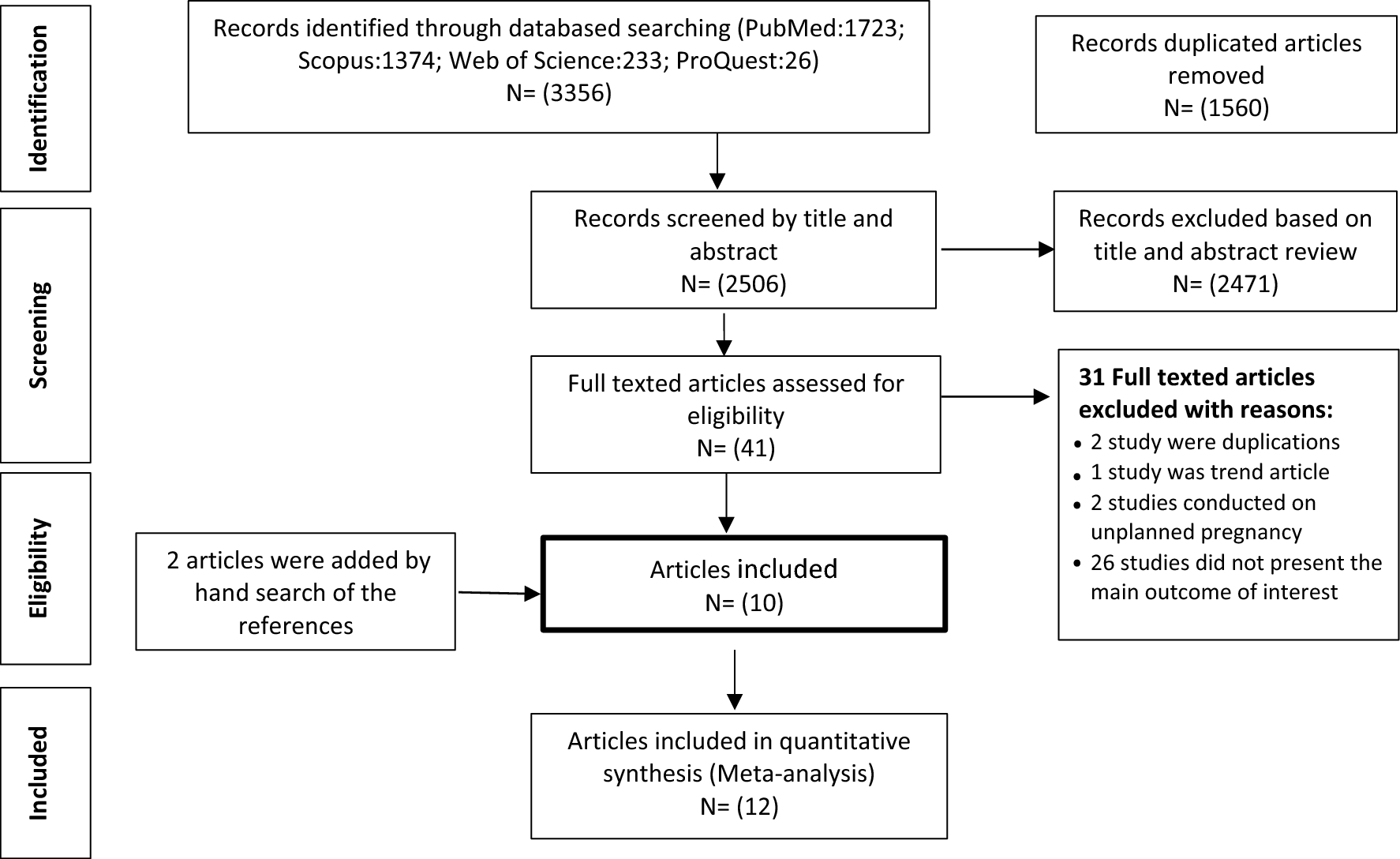

Thirty in-depth interviews were conducted with the key stakeholders. The mean age of the participants was 49.5 years (range: 35-65 years). Most participants (73.4%) held an MD or PhD degree. Four participants worked in MOHME, 12 in medical universities, and 14 in hospitals; more than half had over 20 years of work experience (Table 2).
Table 2 Demographic characteristics of the key stakeholder participants (n=30)The identified challengesThe challenges of implementing each intervention (currently implemented in the system) were identified and categorized using the domains and constructs/sub-constructs of the CFIR (Table 3).
Table 3 Challenges of implementation of a multi-level intervention to reduce mistreatment of women during childbirth; CFIR domains and constructs/ sub-constructsIndividual-level interventionsAt the individual level, two interventions were listed according to the determinants of mistreatment based on the model: childbirth preparation classes and the presence of birth companions (Fig. 1). Both interventions are implemented in the system; however, there were serious challenges in the settings, as outline below.
Training of pregnant women about the process of labour and childbirth, respectful care and their rights during childbirthIn our study, participants shared opinions about the challenges of implementing childbirth preparation classes in five CFIR domains (intervention characteristics, outer setting, inner setting, characteristics of individuals involved, and process of implementation).
Intervention characteristicsAdaptabilityThe level of adaptability of the intervention (childbirth preparation classes) was described as a key barrier to its implementation by most participants. They believed that non-compliance of the conditions and facilities of maternity hospitals with the educational content of the classes, improper timing of the start of classes (from the 20th week of pregnancy), and poor announcements can weaken the implementation of the intervention. The participants suggested that for effective childbirth preparation classes, the situations of facilities of maternity hospitals can be tailored and refined according to the educational content of the classes. Additionally, classes should be held in the early phases of pregnancy and widely announced.
“The training that women receive in classes is different from that implemented in maternity hospitals. For example, we teach that they can move during labour, take their preferred position during childbirth, and have a chosen companion. However, in practice, this has not been implemented in maternity hospitals ...” (Reproductive Health Specialist, University level)
“Announcing about childbirth preparation classes in hospitals and health centers is poor. Only 18% of the pregnant women participated in classes. We did not announce them correctly…” (Health Policy Specialist, MOHME level)
Design quality and packagingWeakness in the design quality and packaging of childbirth preparation classes prevent their successful implementation. Some participants (obstetricians) reported a lack of a multidisciplinary team in holding classes as a barrier to implementation. They believed that classes should be managed by a team and should not be exclusive to midwives. However, the midwives stated that the content of the classes was such that it could be handled by them, but the presence of a psychologist in some sessions could play an important role in the success of the classes.
“We must accept that midwives cannot cover all sessions. Psychologists, nutritionists, and obstetricians can be used in these classes.” (Obstetrician, Hospital level)
Outer settingPatient needs and resourcesLack of training about RMC was also considered a fundamental factor. Most participants highlighted that women do not understand respectful care principles and their rights during childbirth, and this should be integrated into the content of childbirth preparation classes.
“… They should be aware of their rights during childbirth. This should be integrated into the content of the childbirth preparation classes.” (Obstetrician, MOHME level)
CosmopolitanismA crucial factor affecting childbirth preparation class implementation was the poor collaboration of the private sector to hold classes. Participants reported that since most pregnant women receive their care from the private sector (obstetricians and/or midwives' offices), there is a need to establish efficient mechanisms for more support and collaboration of these sectors in holding classes.
“Participation of the private sector is essential because 70% of pregnant women receive their care from obstetricians and midwives.” (Midwife, University level)
Inner settingOrganizational incentives and rewardsA few participants expressed concerns about the poor implementation of childbirth preparation classes following the low participation of pregnant women in classes. They believed that setting enough incentives could affect women’s degree of engagement and commitment to participate in classes.
“Between 9-10% of pregnant women attend our classes (health centers), and this rate is very low ... If incentives are provided, they are more motivated to participate.” (Reproductive Health Specialist, University level)
Available resourcesParticipants reported that poor physical environment and staff shortages were barriers to implementing childbirth preparation classes.
“In some hospitals, there is no standard space to hold classes, especially in private hospitals.” (Midwife, Hospital level)
“Dedicated instructors should be considered in these classes. Here, they appoint one person as an instructor, and at the same time, she has to work shifts in the maternity hospital because they do not have staff.” (Midwife, Hospital level)
Characteristics of individuals involvedOther personal attributesInstructors’ skill and interest was another challenge that was highlighted by some participants: “Unfortunately, some of our midwives (as instructors of classes) are rarely interested in training or do not have enough skills …” (Reproductive Health Specialist, Hospital level)
Process of implementationExecutingPoor execution of childbirth preparation classes, especially during the COVID-19 pandemic, was an important challenge discussed by participants. They also believed that focusing on quantity and neglecting the quality of the classes made them not have the proper efficiency, and their goal was rarely reached: “The classes are implemented, but they are not implemented according to plan and properly ... Unfortunately, we focused on the quantity of the classes, for example, the forms we have to complete and the statistics we have to give to the MOHME.” (Reproductive Health Specialist, University level)
Reflecting and evaluatingSupervising implementation and continuous evaluation were crucial factors emphasized by the participants. They acknowledged that the MOHME should supervise the implementation of childbirth preparation classes in hospitals and health centers through regular inspections. In addition, evaluate the progress and quality of their implementation through an external evaluation.
“I think the biggest challenge of childbirth preparation classes is that there is no supervision of their implementation … There should be a monitoring and auditing system.” (Reproductive Health Specialist, MOHME level)
Presence of birth companionsIn this study, the challenges of implementing birth companions in four CFIR domains (outer setting, inner setting, characteristics of individuals involved, and process of implementation) were discussed by the participants.
Outer settingPatient needs and resourcesAccording to the participants, the lack of knowledge of companions could be a barrier to their attendance at maternity hospitals. Some participants believed that a person going to be a birth companion should be required to participate in childbirth preparation classes and receive training:
“Companions have limited knowledge. I think birth companions should be required to participate in childbirth preparation classes because those who are trained in these classes are helpful to both labouring women and us providers.” (Reproductive Health Specialist, Hospital level)
Inner settingStructural characteristicsThe lack of physical space in some maternity hospitals was another factor that some participants stated: “Some of our maternity hospitals do not have a standard structure, for example, Hospital X, which is a hall with 12 beds and set up some extra beds because of the high visits, so there will be no place for the presence of a birth companion.” (Health Policy Specialist, MOHME level)
CultureThe participants also reported cultural issues as barriers to the implementation of birth companions. They noted that most of the time, if the companion is a partner, due to the feminine environment of maternity hospitals and female providers’ unwillingness to be accompanied by men in the delivery room; they are not allowed to be accompanied.
“The companion is not allowed to enter the maternity hospital; why? Because my colleague (midwife or doctor) does not like a man to be in the labour room, she says, 'No, sir, you go out and let a woman come.” (Reproductive Health Specialist, MOHME level)
CompatibilityOne potential barrier to implementation was concern about the compatibility of the presence of birth companions with the existing workflows of maternity staff. The participants agreed that the interference of birth companions in the clinical duties of staff was a major factor for not allowing a companion.
“As a midwife who worked in a maternity hospital for several years and was strongly against the presence of birth companions, I say that our main challenge was the interference of companions. For example, when a labouring woman's serum runs out, the companion comes many times and warns …” (Midwife, University level)
Characteristics of individuals involvedOther personal attributesSome participants believed that the unwillingness of staff was an important barrier. They mentioned that staff prevents the presence of birth companions because of the perception that the companion is witnessing their performance as an advocate for the woman, which may cause them to expect more attention to labouring women.
“The companion is like an advocate; it is like a hidden camera. Why do some staff members not like companions to enter maternity hospitals? This is because it controls their performance …” (Obstetrician, Hospital level)
Process of implementationReflecting and evaluatingAnother factor was related to lack of supervision. The participants highlighted the need for continuous supervision of the implementation of birth companion guidelines in hospitals: “The presence of birth companions has a guideline that has been communicated to all hospitals, but in many hospitals, especially public hospitals, it is not implemented because it is not supervising ...” (Obstetrician, University level)
Healthcare provider-level interventionAt this level, five interventions were listed according to the determinants of mistreatment based on the model (Fig. 1). However, one of them (integrating RMC into the in-service training of maternity staff) is implemented in the system. The challenges of this intervention were identified as follows:
Integrating RMC into in-service training of maternity staffParticipants in this study reported intervention implementation challenges in the four CFIR domains (outer setting, inner setting, characteristics of individuals involved, and process of implementation).
Outer settingExternal policies and incentivesRegulations and guidelines related to in-service training of staff affect the quality and efficiency of courses. Weakness in some regulations and guidelines has caused staff to be given a quantitative view, which means that many of them participate in the training course to obtain a certificate, rather than improve their knowledge, skills, and behavior, and/or increase the organization's productivity.
“… Unfortunately, our regulations and guidelines are quantitative; that is, they dictate that if a person spends X hours in a year, it will be included in his/her evaluation and career promotion. Therefore, staff members only participate in courses to complete their duty hours and obtain a certificate.” (Midwife, University level)
Inner settingRelative priorityObtaining a license to hold an in-service training course was one of the challenges mentioned by some of the participants. They expressed the belief that the necessity of holding a respectful care training course should be clarified in the steering committee of training and empowerment of human resources in such a way that the course is included in the specialized and mandatory training of employees, not general and optional; thus, it is effective in their career development and they have sufficient motivation to participate in the course.
“One of the challenges is to obtain a license to hold the course. You must justify the necessity of holding a respectful care training course in such a way that the course is included in the job description of the maternity staff.” (Public Health- related manager, University level)
Available resourcesAllocation of an insufficient budget for staff training was an important challenge reported by some participants. They found that staff participation in training courses required more financial support: “Unfortunately, the investment in training staff is very low. The per capita education budget for healthcare staff training this year is 800,000 Iranian rials (IRR), is very small.” (Public Health- related manager, MOHME level)
Similarly, the lack of experienced instructors is considered a challenge. When the instructor of an in-service training course does not have specialized knowledge and teaching ability, the course does not have the necessary efficiency and is not welcomed.
Access to knowledge and informationThe participants also believed that informing the staff about the value and importance of the training course played an important role in its successful implementation. They highlighted that information and materials about the importance of RMC should already be provided to the maternity staff. A participant said: “First, it clarifies the importance of respectful care training for the maternity staff. They need to know how much their behavior with labouring women can affect their mental health status as well as their decisions for future pregnancies.” (Health Services Management Specialist, University level)
Characteristics of individuals involvedKnowledge and beliefs about the interventionManagers do not believe in in-service training for staff, and lack of support for them has caused the need for this training to not be included in the organization's plans and priorities.
“Some managers do not support participation in training courses, and they do not believe that these courses have many benefits for the individual and organization.” (Public Health- related manager, University level)
Process of implementationReflecting and evaluatingAnother major challenge was the weakness of evaluating the effectiveness of the training courses. The participants acknowledged that, although the evaluation of the effectiveness of courses is done using Kirkpatrick's model [47], it is often incomplete or limited to the first two levels of this model, and the third and fourth levels are not done because of problems and complexity.
“... Our current evaluation method is flawed, and we do not evaluate almost any of our courses at the level of behavior; therefore, we cannot be sure if the person who participated in the course acquired the expected capabilities.” (Reproductive Health Specialist, University level)
Hospital-level interventionAt the hospital level, four interventions were listed based on the model (Fig. 1). Of these, the evaluation of the performance of MHCPs is implemented in the system. The identified challenges for this intervention were as follows:
Evaluating the performance of MHCPs about mistreatment and/or RMCIn our study, participants discussed the intervention implementation challenges in two CFIR domains (outer setting and process of implementation).
Outer settingExternal policies and incentivesSome participants complained of weakness in laws and regulations. They stated that to supervise the performance of MHCPs in laws and regulations (including the Support of Family and Youth Population Act), the merit pay of providers dependent on the satisfaction of pregnant women is defined. However, they are not included in the payment systems of all MHCPs. Furthermore, participants expressed concern that these laws (such as reducing merit pay or warnings) were not very effective in supervising the performance of the providers.
“Currently, in the Support of Family and Youth Population Act, merit pay of the providers depends on the satisfaction of pregnant women, but unfortunately not for all providers (including obstetricians or residents). We are pursuing this to be modified.” (Health Policy Specialist, MOHME level)
Process of implementationExecutingPoor execution of the intervention (mother’s satisfaction questionnaire) was considered important. Participants stated that, although all hospitals were required to implement and provide feedback to the MOHME, the providers often completed the questionnaire. To solve this problem, an electronic satisfaction questionnaire is currently being designed, whose links will be sent to women, and their satisfaction reports will be registered in the Ministry of Health's portal. However, owing to the poor support of the Information Technology (IT) unit, it has not yet been implemented.
“… Unfortunately, the questionnaires were completed by the providers, without the mother being informed. Currently, an electronic questionnaire is designed, the report of which will be registered in the Ministry of Health's portal, but it has not yet been implemented.” (Reproductive Health Specialist, Hospital level)
National health system-level interventionAt the national health system level, the implementation of pain relief during childbirth guidelines was listed based on the model (Fig. 1). This intervention is implemented in the system, and its challenges were as follows:
Implementation of pain relief during childbirth guidelinesIn this study, the participants identified implementation challenges in the four CFIR domains (outer setting, inner setting, characteristics of individuals involved, and process of implementation).
Outer settingPatient needs and resourcesParticipants mentioned the lack of knowledge of pregnant women as an important challenge in implementing pain relief during childbirth. They believed that most women are unaware of the option of pain relief during childbirth. Pregnancy is an important time to inform and prepare women about pain relief options during childbirth; however, women are unaware of this right and do not demand it.
“… Pregnant women do not have sufficient information regarding pain relief during childbirth … so they do not demand ... Information about this should be provided during pregnancy (for example, in childbirth preparation classes), but when labouring women come to the maternity hospital, we have to go and explain … I think that this is not the right time for training.” (Anesthesiologist, Hospital level)
Some participants also pointed out that a large number of their clients are Afghan women who refuse pain relief, because they do not have insurance coverage and would be required to pay out-of-pocket.
“... Most of our clients are Afghan women. They do not have insurance and have to pay for it. Therefore, they do not do (pain relief during childbirth).” (Obstetrician, Hospital level)
CosmopolitanismThe presence of good networking and relationships with external organizations, such as insurance organizations, to modify pain relief during childbirth tariffs and motivate staff was described by participants as an effective factor in implementation.
“The support of insurance organizations is also crucial for the implementation of pain relief during childbirth; tariffs should be revised, but unfortunately, they do not collaborate.” (Obstetrician, MOHME level)
External policies and incentivesMOHME policies and support were critical for the successful implementation of pain relief during childbirth. Some participants believed that being free of charge for pain relief during childbirth in public hospitals was one of the factors facilitating its implementation. However, the participants reported that some measures of the MOHME, including the absence of on-call anesthesiologists in hospitals were another challenge for the implementation of the program.
“... The hospital should have an on-call anesthetist, which unfortunately the MOHME took it away ... Therefore; we do not have the possibility of pain relief during childbirth at night because we there is not have an on-call anesthesiologist. There is an aesthesia resident, but it is normal that she/he does not spend X hours on pain relief during childbirth and quickly performs a caesarean section.” (Obstetrician, Hospital level)
Inner settingNetworks and communicationsPoor working relationships between obstetricians and anesthesiologists were key barriers. Some participants believed that obstetricians are the primary decision-makers for pain relief during childbirth, and if they approve, labouring woman will be referred to anesthesiologists, but unfortunately, they do not collaborate enough in this regard. A participant stated:
“Obstetricians should select labouring women based on the criteria and then refer to them. Unfortunately, they do not collaborate with us …” (Anesthesiologist, Hospital level)
Available resourcesThe availability of resources during the implementation process was critical for success. The participants complained about the low tariff allocated to pain relief during childbirth and considered it a fundamental barrier to non-collaboration of anesthesiologists in the implementation of the program. Furthermore, the lack of staff (anesthesiologists and nurse anesthetists) to offer top-ups and continuous monitoring adds to this factor.
“Pain relief during childbirth is a time-consuming process, but the tariff is so low that the anesthesiologist does not want to perform it. However, there is a shortage of anesthesiologists and nurse anesthetists in most hospitals.” (Anesthesiologist, Hospital level)
Access to knowledge and informationSimilarly, limited access to knowledge and information about pain relief during childbirth for the provider team was considered another challenge. The participants identified a lack of adequate training for providers prior to implementing the program as a contributing factor.
“Prior to the implementation of this program (pain relief during childbirth), sufficient training should have been provided to all team members (including anesthesiologists, obstetricians, and midwifes), and the purpose and importance of the program were well introduced. We were not justified at all as to why we wanted to do this program ...” (Obstetrician, Hospital level)
Characteristics of individuals involvedKnowledge and beliefs about the interventionAnother challenge was the lack of knowledge and misconceptions of providers (obstetricians and midwives) regarding pain relief during childbirth. For example, it is believed that pain relief during childbirth is associated with an increased risk of prolonged labour, poor maternal and infant outcomes, and an increased chance of cesarean section. The participants believed that there was a serious need to spread awareness and cultivate a positive attitude among providers about the benefits of pain relief during childbirth and eliminate misconceptions by holding training courses.
“I think the most important challenge is misconceptions. Still, many obstetricians do not agree with pain relief during childbirth; it is believed that it prolongs the labour process or may have complications for the mother and/or the infant; all this is due to lack of knowledge. This belief needs to be corrected.” (Anesthesiologist, Hospital level)
Other personal attributesAccording to most participants, the lack of expertise and skills of anesthesiologists was another barrier to implementation. They acknowledged that pain relief during childbirth is one of the important abilities that anesthesia residents should acquire, which has not been considered in their educational curriculum. Anesthesiology residents spend a short period of one month in the maternity ward, so they do not acquire enough skills.
“Pain relief during childbirth requires expertise and skill ... However, it has not been considered an important topic in the educational curriculum of anesthesiologists.” (Midwife, University level)
Process of implementationExecutingSome participants felt that pain relief during childbirth had not been implemented according to the implementation plan. They emphasized the identification of program problems and the importance of proper planning: “At first, the process of pain relief during childbirth in our hospitals was increasing; for example, in our hospital, we had about 500 pain relief during childbirths per month, but currently we do not have four ... We were weak in execution; we have implemented the program since 2014, but unfortunately, I can say that we have been unsuccessful thus far.” (Anesthesiologist, Hospital level)
Reflecting and evaluatingIn addition, supervising the implementation of pain relief during childbirth in hospitals was another factor mentioned by some participants. They stated that internal and external inspections should be used to supervise the performance of the team in providing pain relief during childbirth.
“There must be supervision ... If it is not done (pain relief during childbirth), it is not supervised that why was it not done? The mother did not request or you (providers) did not?” (Health Education and Promotion Specialist, University level)
留言 (0)