Previous studies have provided evidence supporting the effectiveness of combining rh-endostatin with chemotherapy in improving PFS and OS in patients with advanced NSCLC [15, 20]. However, there is limited data available on the use of a 5-day intravenous infusion of rh-endostatin in combination with chemotherapy as a first-line treatment for advanced NSCLC. Therefore, this prospective study aimed to optimize the dosing regimen of rh-endostatin for previously untreated advanced NSCLC patients and evaluate the efficacy and safety of this treatment approach when combined with chemotherapy. The studys findings illustrated that the mPFS and mOS of NSCLC patients receiving this treatment regimen were enhanced. In addition, the toxicities were deemed acceptable and manageable. Overall, these findings add to the expanding body of evidence that supports the effectiveness and safety of combining a 5-day continuous intravenous infusion of rh-endostatin with chemotherapy as a viable first-line treatment for advanced NSCLC patients. To the best of our knowledge, this is the first prospective study investigating the use of a 5-day intravenous infusion of rh-endostatin in combination with chemotherapy as a first-line treatment for advanced driver gene-negative NSCLC.
In the current clinical practice, a combination therapy of anti-programmed cell death 1 (PD-1)/programmed cell death ligand 1 (PD-L1) antibodies and platinum-based chemotherapy has emerged as a widely employed first-line treatment for patients with advanced NSCLC that is unresectable and lacks driver mutations [24, 25]. In March 2019, the National Medical Products Administration (NMPA) of China approved the use of Opdivo and Keytruda in combination with chemotherapy as the first-line treatment for metastatic nonsquamous NSCLC in patients without EGFR and ALK mutations. However, due to the accessibility and expense of PD-1 antibodies, they were not included in our study. According to the IMpower150 study, the addition of atezolizumab to bevacizumab plus chemotherapy showed a significant improvement in PFS and OS among patients with metastatic nonsquamous NSCLC, regardless of their PD-L1 expression and EGFR or ALK genetic alteration status [26]. Therefore, our study offers an alternative treatment approach that combines PD1/PD-L1 inhibitor therapy for NSCLC patients without driver mutations, particularly for those with squamous NSCLC.
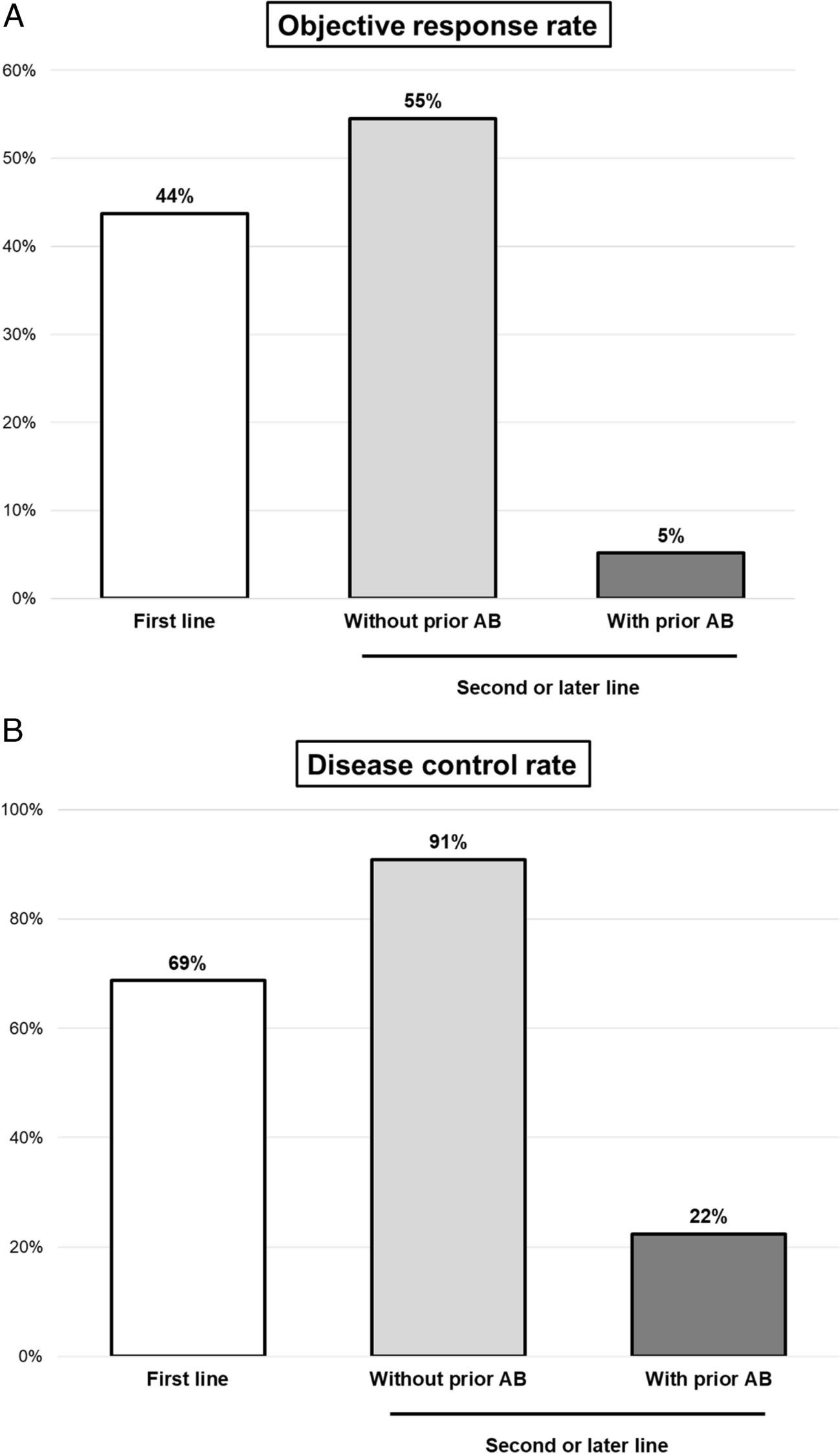
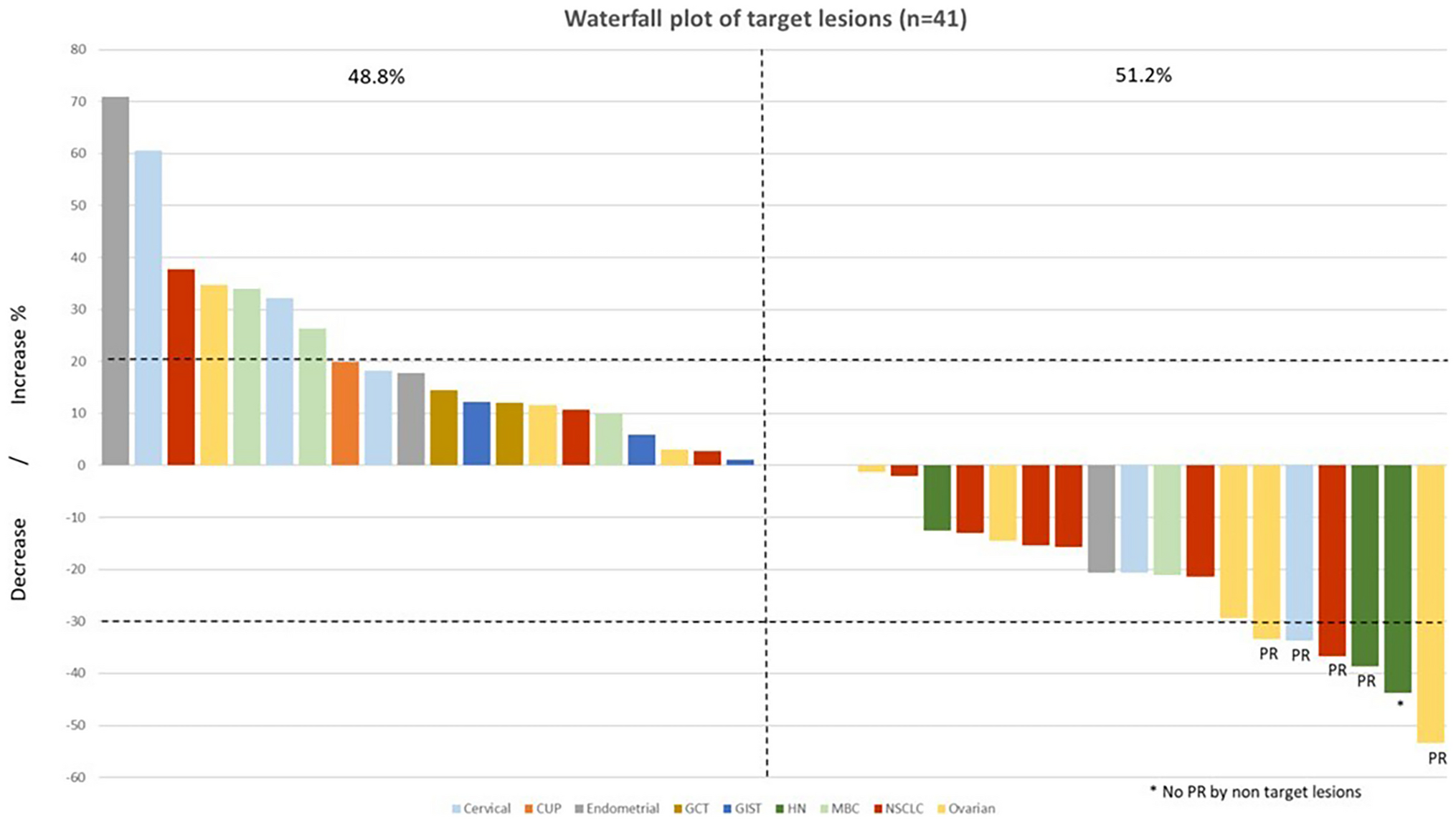
The results of this study demonstrated an ORR of 52.1% and a DCR of 75.0%. These findings are consistent with a study conducted by Sun et al., which examined the use of rh-endostatin combined with NP (vinorelbine + cisplatin) in NSCLC patients for the first time. They reported a response rate of 40% and a clinical benefit rate of 76.52% [15]. In a study by Cheng et al., the ORR and DCR for the continuous intravenous infusion of rh-endostatin in combination with first-line chemotherapy were 40.0% and 65.0%, respectively [27]. Furthermore, results from a large phase II clinical trial led by Han et al. revealed an ORR of 39.3% and a DCR of 90.2% in patients treated with rh-endostatin and paclitaxel-carboplatin (TC) [16]. In terms of prognosis and survival, Sun et al. reported a median time to progression of 6.3 months and a mOS of 13.75 months [15]. Han et al. reported that the mPFS and mOS were 7.1 versus 6.3 months (p = 0.522), and 17.6 versus 15.8 months (p = 0.696) in the treatment (TC + rh-endostatin) and control groups (TC + placebo), respectively [16]. Another study comparing different administration methods of rh-endostatin in NSCLC treatment demonstrated a mPFS of 6.0 months for patients receiving continuous intravenous infusion of rh-endostatin [27]. These results are in line with our findings in the present study.
Continuous intravenous infusion of rh-endostatin has been shown to extend the drug’s circulation time in the bloodstream and enhance its anti-tumor activity [28]. The use of portable infusion pumps for 120 h allows for continuous administration, ensuring that the anti-angiogenic treatment improves the accessibility of chemotherapy drugs to tumor cells [22]. In a study by Hansma et al., the safety of different doses of rh-endostatin was compared. It was found that a continuous intravenous infusion of rh-endostatin (210 mg) for 120 h was well-tolerated and related to the optimal time window for vascular normalization [22]. Furthermore, a study compared the efficacy and safety of continuous versus intermittent intravenous infusion of rh-endostatin in combination with chemotherapy for advanced NSCLC. The results revealed similar PFS and ORR between continuous and intermittent intravenous infusion of rh-endostatin (210 mg) [27]. Based on these findings, it can be concluded that a continuous intravenous infusion of rh-endostatin at a dose of 210 mg for 120 h is a feasible treatment regimen.
The combination of rh-endostatin and chemotherapy can result in common adverse reactions such as leukopenia, anemia, decreased appetite and hypertension [29]. In this study, grade 3–4 adverse reactions mainly consisted of leukopenia(6.3%), anemia(2.1%), and thrombocytopenia(2.1%) which were primarily related to chemotherapy. Similar grade 3–4 adverse reactions, including granulocytopenia (25.0%), anemia (5.0%), and thrombocytopenia (10.0%), were the most common in the study by Cheng et al. [27]. A meta-analysis indicated that angiogenesis inhibitors can potentially result in adverse reactions such as hypertension and myocardial ischemia [30], however the above adverse reactions were not observed in our study. Overall, the adverse events reported in the present study were manageable.
Rh-endostatin primarily targets the blood vessels of tumors rather than the tumor cells themselves. As a result, responsive patients may not experience immediate changes in tumor size following drug administration [31]. Identifying patients who will benefit from rh-endostatin is of utmost importance. Currently, there are no accurate predictors available to forecast the efficacy of rh-endostatin, although certain serum markers such as CEA and LDH have been proven to predict the efficacy of bevacizumab [32,33,34]. Gerald et al. confirmed that a high baseline CEA serum level predicted a poor outcome in patients with advanced colorectal cancer treated with bevacizumab [32]. In our study, we found that a low baseline CEA level was strongly associated with a longer PFS in NSCLC patients treated with rh-endostatin and chemotherapy. This finding is significant as it suggests that CEA levels could potentially serve as an outcome measure marker for rh-endostatin treatment in NSCLC patients. The possible reason behind this association is that overexpression of CEA enhances tumor angiogenesis. CEA induces pro-angiogenic behaviors in endothelial cells, including adhesion, spreading, proliferation, and migration in vitro, as well as tumor microvascularization in vivo independently of the vascular endothelial growth factor (VEGF)/VEGF receptor (VEGFR) system [35].
While this study provided valuable findings, it does have limitations. Firstly, the sample size was relatively small, although it was deemed sufficient to establish the conclusions of this study. However, larger sample sizes in future studies would provide more robust evidence. Secondly, this study was a single-arm study and did not include a control group for comparison. While comparing results with previous studies can offer some support for our conclusions, it is necessary to conduct controlled trials with larger sample sizes to validate our findings. Addressing these limitations through larger controlled trials would further strengthen the reliability and generalizability of the conclusions drawn from this study.





留言 (0)